.jpg)
Mandibular Desmoplastic Ameloblastoma - Case Report And Brief Literature Review
Bruno Teixeira Gonçalves Rodrigues1*  , Paula Granha Porto1 , Danilo Passeado Branco Ribeiro 2 , Marcele Cruz da Silva2 and Mônica Simões Israel3
, Paula Granha Porto1 , Danilo Passeado Branco Ribeiro 2 , Marcele Cruz da Silva2 and Mônica Simões Israel3
1Department of Oral Medicine, Faculdade São Leopoldo Mandic, Rio de Janeiro, Rio de Janeiro, Brazil .
2Oral and maxillofacial surgery, Rio de Janeiro State University, Rio de Janeiro, Rio de Janeiro, Brazil .
3Oral Medicine, Department of Diagnosis and Therapeutics, Rio de Janeiro State University, Rio de Janeiro, , Rio de Janeiro, Brazil .
http://dx.doi.org/10.12944/EDJ.08.0102
Desmoplastic ameloblastoma (DA) accounts for 4–13% of all ameloblastomas and presents unique characteristics, such as the ability to appear as a mixed radiolucent–radiopaque image radiographically, differing from the typically radiolucent appearance of CA. The biological behavior of DA is like that of other CA variants and therefore should be treated similarly. The present study, reported a case of DA affecting a young female, highlighting its clinical, radiographic and treatment outcomes. Intraorally, a firm submucosal enlargement was observed in the anterior mandibular area. Radiographically, a radiolucency was observed between the the lower left lateral incisor and canine teeth. An incisional biopsy was performed, confirming the histopathological diagnosis of DA. The patient was submited to radical surgery under general anesthesia and there are no signs of the tumor after a 2-year follow-up. Therefore, the present case demonstrated the importance of early diagnosis and appropriate radical surgical management, which allowed effective tumor control with preservation of mandibular integrity and satisfactory functional outcome, with no recurrence after two years.
Copy the following to cite this article:
Rodrigues B. T. G, Porto P. G, Ribeiro D. P. B, Silva M. C. D, Israel M. S. Mandibular Desmoplastic Ameloblastoma - Case Report and Brief Literature Review. Enviro Dental Journal 2026;8(1).
DOI:http://dx.doi.org/10.12944/EDJ.08.0102Copy the following to cite this URL:
Rodrigues B. T. G, Porto P. G, Ribeiro D. P. B, Silva M. C. D, Israel M. S. Mandibular Desmoplastic Ameloblastoma - Case Report and Brief Literature Review. Enviro Dental Journal 2026;8(1). Avialable here: https://bit.ly/3MxMGnQ
Download article (pdf) Citation Manager

Introduction
Conventional ameloblastoma (CA), a locally aggressive epithelial odontogenic tumor (OT), accounts for 11–59% of all OTs and shows a predilection for the posterior mandibular region.1-2 Histologically, CA is classified into follicular, plexiform, acanthomatous, basal cell, granular, and, on rare occasions, desmoplastic subtypes.1-4
Desmoplastic ameloblastoma (DA) accounts for 4–13% of all ameloblastomas and presents unique characteristics, such as the ability to appear as a mixed radiolucent–radiopaque image radiographically, differing from the typically radiolucent appearance of CA.5 Moreover, microscopic findings are essential for establishing the diagnosis of DA and distinguishing it from other CA subtypes. Histopathological examination is characterized by odontogenic epithelium within a dense desmoplastic stroma.1-4
The biological behavior of DA is like that of other CA variants and therefore should be treated similarly.5 Radical surgery with bone resection is indicated to prevent recurrence and reduce the risk of malignant transformation.1-4
Herein, we report a case of DA affecting the anterior mandible region of a young female, highlighting its clinical, radiographic, and treatment outcome features.
Case Report
A 25-year-old female was referred for evaluation of a three-month history of an asymptomatic intraoral swelling in the anterior mandibular region. The patient’s medical history was unremarkable, and she denied tobacco and alcohol use. Extraoral examination revealed a slight facial volume growth in the inferior anterior region (Figure 1A). Intraorally, a firm submucosal swelling extending from the mandibular midline to the left mandibular canine was observed (Figure 1B).
Orthopantomography revealed an ill-defined, multilocular radiolucency in the anterior mandible, causing root divergence of the left mandibular lateral incisor and canine (Figure 1C). Cone-beam computed tomography (CBCT) scans demonstrated a large hypodense lesion associated with cortical expansion and resorption (Figure 1D-E). Pulp vitality testing of the involved teeth yielded positive results.
Therefore, ameloblastoma, odontogenic myxoma, odontogenic keratocyst and central giant cell lesion were included in the clinical differential diagnosis. An incisional biopsy was performed under local anesthesia (aspiration was negative, suggesting a solid lesion), and the specimen was submitted for analysis. Histological exam revealed compressed epithelial islands and peripheral palisading of columnar ameloblastic cells and loosely arranged central cells were observed, all embedded within a dense desmoplastic stroma, establishing the diagnosis of desmoplastic ameloblastoma.
The patient was submitted to surgical treatment, and marginal resection of the lesion was performed under general anesthesia (Figure 2A-C). Recovery was uneventful, and there are no signs of the tumor after a two-year period (Figure 2D-E).
.jpg) | Figure 1: A, Extraoral examination demonstrating mild facial volume growth. B, Intraorally, showing an asymptomatic volume growth located in the anterior mandible. C, Panoramic radiograph revealing an ill-defined, multilocular radiolucency located between the left mandibular lateral incisor and canine, with associated root divergence.
|
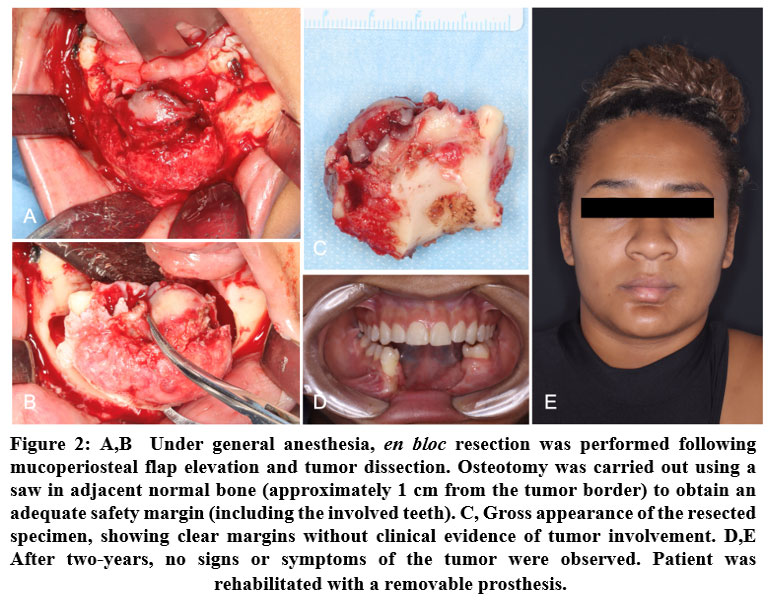 | Figure 2: A,B Under general anesthesia, en bloc resection was performed following mucoperiosteal flap elevation and tumor dissection. Osteotomy was carried out using a saw in adjacent normal bone (approximately 1 cm from the tumor border) to obtain an adequate safety margin (including the involved teeth).C, Gross appearance of the resected specimen, showing clear margins without clinical evidence of tumor involvement. D,E After two-years, no signs or symptoms of the tumor were observed. Patient was rehabilitated with a removable prosthesis.
|
Discussion
First described by Eversole et al.6 in 1984 as a new variant of ameloblastoma—alongside unicystic, peripheral, and metastatic types—the most recent classification of head and neck tumors by World Health Organization (WHO)? now includes desmoplastic ameloblastoma (DA) solely as a histopathological subtype of ameloblastoma.
Conventional ameloblastoma predominantly affects the mandible rather than the maxillary region, with a ratio of approximately 5:1, most commonly involving the posterior region.8 A slight male predilection has been reported, and the tumor typically occurs between the third and fifth decades of life. In contrast, DA more frequently arises in the anterior region of the jaws and shows no significant difference in prevalence between the superior and lower jaw. Additionally, DA demonstrates a slight female predilection,9 with a reported age range between 16 and 75 years.1,2 The present case describes a desmoplastic ameloblastoma occurring in a 25-year-old female in the anterior mandibular region, which is consistent with previously reported findings in the literature.
Radiographically, DA may exhibit a pattern distinct from other ameloblastoma subtypes, often presenting as a mixed radiolucent–radiopaque image.1-6 Previous studies have demonstrated that approximately 55% of cases present as mixed lesions,10 whereas others may appear solely radiolucent, as observed in the present case. Moreover, in contrast to CA, the desmoplastic variant is frequently characterized by an ill-defined radiolucent appearance rather than the well-defined margins commonly seen in most ameloblastomas.1 This imaging pattern is particularly important in lesion assessment, as it may mimic fibro-osseous lesions. Consequently, in the differential diagnosis of radiolucent–radiopaque lesions of the jaws, DA should be included.
The therapeutic approach to ameloblastoma is determined by the tumor subtype and its extent.1-6 Unicystic and peripheral variants are generally managed with conservative procedures, whereas conventional ameloblastoma typically requires more aggressive treatment. Similarly, desmoplastic ameloblastoma is best managed with radical surgical intervention,11 as conservative approaches, such as curettage, have been associated with increased recurrence rates. Consequently, radical procedures, including segmental resection, are considered to provide better local control, although they frequently necessitate plate fixation or more complex reconstructive techniques.12 In the present case, radical surgical management was chosen, and en bloc resection was feasible due to the limited size of the tumor, allowing preservation of the inferior border of the mandible without the need for plate fixation. Nevertheless, the patient was maintained on a liquid diet for one month postoperatively to minimize the risk of pathological fracture.
Conclusion
Desmoplastic ameloblastoma is a relatively rare histopathological subtype of ameloblastoma that presents distinct clinical, radiographic, and microscopic features, often posing diagnostic challenges. Its tendency to occur in the anterior regions of the jaws and to exhibit radiolucent/radiopaque appearance may mimic other fibro-osseous lesions, reinforcing the importance of thorough radiographic evaluation and histopathological confirmation. DA requires an equally aggressive surgical approach due to its infiltrative growth pattern and potential for recurrence. The present case demonstrated the importance of early diagnosis and appropriate radical surgical management, which allowed effective tumor control with preservation of mandibular integrity and satisfactory functional outcome, with no recurrence after two years.
Acknowledgement
The authors gratefully acknowledge the Oral Pathology service of Rio de Janeiro State University Dental School for the microscopic analysis and diagnosis of the case.
Funding Sources
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of Interest
The author(s) declares no conflict of interest.
Data Availability Statement
This statement does not apply to this article.
Ethics Statement
This case report was not part of a full research that requires ethical approval.
Informed Consent Statement
The informed consent was obtained from the patient and it is in accordance to the standards currently applied in Brazil.
Clinical Trial Registration
This research does not involve any clinical trials.
Permission to Reproduce Material from other Sources
None included.
Author Contributions
Rodrigues B.T.G - Conceptualization, writing - original draft;
Porto P.G - writing - original draft;
Ribeiro D.P.B, Cruz M. and Israel M.S - writing - original draft, review and editing.
References
- Sharma A, Ingole S, Deshpande M, Meshram D. Retrospective analysis of Desmoplastic Ameloblastoma: Clinical review. Med Oral Patol Oral Cir Bucal. 2021;26(2):e246-e255.
CrossRef - Waldron CA, el-Mofty SK. A histopathologic study of 116 ameloblastomas with special reference to the desmoplastic variant. Oral Surg Oral Med Oral Pathol. 1987;63(4):441-451.
CrossRef - Philipsen HP, Reichart PA, Takata T. Desmoplastic ameloblastoma (including "hybrid" lesion of ameloblastoma). Biological profile based on 100 cases from the literature and own files. Oral Oncol. 2001;37(5):455-460.
CrossRef - Hirota M, Aoki S, Kawabe R, Fujita K. Desmoplastic ameloblastoma featuring basal cell ameloblastoma: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005;99(2):160-164.
CrossRef - Savithri V, Janardhanan M, Suresh R, Kumar RV. Desmoplastic ameloblastoma with osteoplasia: Review of literature with a case report. J Oral Maxillofac Pathol. 2013;17(2):298-301.
CrossRef - Eversole LR, Leider AS, Strub D. Radiographic characteristics of cystogenic ameloblastoma. Oral Surg Oral Med Oral Pathol. 1984;57(5):572-577.
CrossRef - Soluk-Tekkesin M, Wright JM. The World Health Organization Classification of Odontogenic Lesions: A Summary of the Changes of the 2022 (5th) Edition. The World Health Organization Classification of Odontogenic Lesions: A Summary of the Changes of the 2022 (5th) Edition. Turk Patoloji Derg. 2022;38(2):168-184.
CrossRef - Reichart PA, Philipsen HP, Sonner S. Ameloblastoma: biological profile of 3677 cases. Eur J Cancer B Oral Oncol. 1995;31B(2):86-99.
CrossRef - Anand R, Sarode GS, Sarode SC, et al. Clinicopathological characteristics of desmoplastic ameloblastoma: A systematic review. J Investig Clin Dent. 2018;9(1):10.1111/jicd.12282.
CrossRef - Mehlisch DR, Dahlin DC, Masson JK. Ameloblastoma: a clinicopathologic report. J Oral Surg. 1972;30(1):9-22.
- N. Wankhede, R. Moharil, A. Dive, S. Khandekar, Desmoplastic ameloblastoma, Ind. J. Appl. Res. 5 (9) (2015) X21–X2
- Nunes LA dos S, Rodrigues BTG, Antero SA, Freire N de A, Israel MS. Conservative Approach of an Unicystic Ameloblastoma on a Young Patient - Case Report. Rev Bras Odontol. Published onlin
CrossRef





