.jpg)
Evidence on the Use of Propolis Gel in the Management of Periodontal Disease: A Narrative Review
Ana Carolina Duarte Firmino  , Nathalya Maria Vilela Moura and Mario Taba Jr*
, Nathalya Maria Vilela Moura and Mario Taba Jr*
1Department of Oral and Maxillofacial Surgery, and Periodontology, School of Dentistry of Ribeirao Preto, University of Sao Paulo, Ribeirao Preto, SP Brazil .
http://dx.doi.org/10.12944/EDJ.08.0105
Natural bioactive compounds have attracted increasing interest as adjuncts in periodontal therapy due to their potential to modulate inflammation and microbial activity. Among these compounds, propolis has been extensively explored because of its antioxidant, antimicrobial, and immunomodulatory effects. The development of gel-based delivery systems has further enhanced its therapeutic potential by enabling localized application and controlled release at periodontal sites. Therefore, this narrative review aimed to summarize and discuss the available scientific evidence regarding the use of propolis-based gels in the treatment of periodontal disease. A total of ten studies were selected from the literature, including in vitro and in vivo investigations (n = 7) and clinical trials (n = 3). Overall, the studies demonstrated that propolis gels exhibited favorable physicochemical properties for periodontal application and suggested potential anti-inflammatory effects. However, the antimicrobial effectiveness against Porphyromonas gingivalis and the reduction in probing depth in animal models presented inconsistent findings. Although clinical studies reported favorable outcomes, substantial methodological heterogeneity among them limits direct comparison and interpretation. In summary, while propolis-based gels show promise as periodontal adjuncts due to their physicochemical properties and anti-inflammatory potential, clinical evidence remains limited and inconsistent. High-quality randomized controlled trials are essential to establish standardized protocols and confirm long-term safety and efficacy.
Copy the following to cite this article:
Firmino A. C. D, Moura N. M. V, Jr M. T. Evidence on the Use of Propolis Gel in the Management of Periodontal Disease: A Narrative Review. Enviro Dental Journal 2026;8(1).
Copy the following to cite this URL:
Firmino A. C. D, Moura N. M. V, Jr M. T. Evidence on the Use of Propolis Gel in the Management of Periodontal Disease: A Narrative Review. Enviro Dental Journal 2026;8(1). Available here:https://bit.ly/4rw9rXH
Download article (pdf) Citation Manager

Introduction
Periodontal disease (PD) is a chronic inflammatory condition with a global prevalence of about 11%, and if left untreated, it can lead to tooth loss and significantly impair quality of life1-3. Among the available treatment options, non-surgical periodontal treatment (NSPT) - based on the mechanical removal of biofilm and calculus, combined with risk factor control and improved oral hygiene - is considered the gold standard. However, its effectiveness is limited in anatomically challenging sites and in patients with systemic conditions that compromise the host response2-4. In this context, adjunctive periodontal therapy (APT) has gained importance for enhancing NSPT outcomes and reducing the need for surgical interventions. Strategies include host modulation, systemic antibiotics, and local approaches such as laser therapy, probiotics, chlorhexidine, and natural products. Locally delivered adjuncts are particularly advantageous due to their targeted delivery and reduced side effects. Innovative drug delivery systems - such as gels, chips, or fibers - are being explored to release active compounds and stabilize the blood clot, underscoring the importance of new treatment options for optimizing PD management3-5.
Among local drug delivery systems, gels stand out as versatile vehicles for periodontal therapy. Gel formulations are three-dimensional networks with bonds between polymeric chains that occur when liquid settles to form a semi-solid. In hydrogels, these polymers are hydrophilic6. Thus, smart hydrogels can change their characteristics based on the microenvironment, such as thermoresponsive hydrogels that undergo sol–gel transition with temperature change, and in situ gels that change their physicochemical characteristics at the target site. These approaches appear to be promising forms of administration, since their formulations can be tailored through rheological properties to achieve the desired injectability5-7.
A wide range of natural and synthetic materials has been explored for gel formulation, offering additional antimicrobial and anti-inflammatory properties. Among them, propolis stands out as a resinous natural substance produced by bees (Apis mellifera) in combination with plant exudates. Its composition varies according to its geographic location and botanical origin. Flavonoids, phenolic acids, waxes, aromatic oils, and pollen are part of its composition4,8. Research indicates that propolis exhibits anti-inflammatory, antimicrobial, and immunomodulatory properties. Propolis helps in the modulation of the immune response by reducing inflammatory cytokines such as interleukin (IL) - IL-1?, IL-1?, IL-4, IL-6, IL-12p40, and IL-12p70, and by increasing serum levels of immunoglobulins like IgA and IgG9. In addition, this substance has been shown to reduce the expression of inflammation-related genes such as Mmp7 and Wnt2b. Moreover, caffeic acid phenyl ester (CAPE) present in propolis may inhibit cyclooxygenase (COX) and lipoxygenase (LOX) activity, reducing prostaglandins and leukotrienes4.
Its antimicrobial effect involves mechanisms such as increasing cell permeability, inhibiting adenosine triphosphate (ATP) production, and interacting with microbial DNA10. It is effective against periodontopathogens such as Porphyromonas gingivalis, Aggregatibacter actinomycetemcomitans, and Prevotella intermedia. Artepillin C has demonstrated bacteriostatic activity against P. gingivalis4. In addition, chrysin and quercetin are flavonoids that have shown effectiveness against alveolar bone resorption, making them useful in the treatment of periodontitis and gingivitis11. Thus, the effects of propolis in the treatment of periodontal disease have been investigated. A systematic review evaluated different propolis administration protocols, including hydroalcoholic solution, and the results demonstrated improvements in periodontal clinical parameters compared to scaling and root planing therapy or placebo12. In this context, the review of strategies for administering propolis specifically incorporated into the form of hydrogels, gels, or thermosensitive hydrogels in the management of periodontitis remains largely unexplored. Therefore, this narrative review aims to clarify the current evidence on propolis-based gels or hydrogels in the context of periodontal diseases, based on in vitro, in vivo, and clinical studies.
Materials and Methods
Study design
This narrative review aims to assess the evidence on the effects of propolis gels in the context of periodontal therapy. Accordingly, the review was structured to address the following question: “What evidence is available regarding the use of propolis gel in the treatment of periodontal disease?”
Search strategy
The literature search was conducted on August 25, 2025, in the Embase, LILACS, Scopus, MEDLINE (PubMed), Web of Science, and SciELO databases. Combinations of descriptors related to propolis (propolis, Brazilian green propolis), delivery systems (hydrogel, gel, thermosensitive, temperature-sensitive, thermoresponsive, mucoadhesive), and periodontal conditions (periodontitis, periodontal disease, periodontal diseases, gingivitis) were used, combined with the Boolean operators AND and OR. No restrictions regarding publication period were applied (Table 1).
Inclusion criteria
The inclusion criteria were defined to select studies that evaluated the use of propolis in gel formulations, including thermosensitive and in situ gels (for the treatment of periodontitis and gingivitis). In vitro studies were included when they involved characteristics relevant to periodontal administration of the gel or periodontal cells/microorganisms. In vivo and clinical studies were also considered, provided they presented outcomes that allowed the evaluation of the effects of propolis on periodontal parameters.
Exclusion criteria
The exclusion criteria included studies conducted in the context of diseases other than periodontitis and gingivitis, such as mucositis, peri-implantitis, and other pathologies of the maxillomandibular complex. Studies employing alternative forms of propolis administration, such as pure extract or gels containing other natural active ingredients, as well as studies in which propolis was used exclusively in combination with other adjunctive therapies or active compounds, were also excluded.
Table 1: Search strategy
Database | Search strategy | Identified records | Date |
Embase | (propolis'/exp OR 'propolis':ab,ti OR 'brazilian green propolis':ab,ti) AND ('hydrogel'/exp OR 'hydrogel':ab,ti OR gel:ab,ti OR 'thermosensitive':ab,ti OR 'temperature-sensitive':ab,ti OR 'thermoresponsive':ab,ti OR 'mucoadhesive':ab,ti) AND ('periodontitis'/exp OR 'periodontal disease'/exp OR 'periodontitis':ab,ti OR 'periodontal disease':ab,ti OR 'periodontal diseases':ab,ti OR 'gingivitis':ab,ti) AND [embase]/lim | 22 | August 25, 2025 |
LILACS | (((propolis) AND (hydrogel OR gel OR termossensível OR thermosensitive OR temperature-sensitive OR thermoresponsive OR mucoadhesive)) ) AND ( ((periodontitis OR periodontal disease OR gengivitis))) AND db:("LILACS") AND instance:"lilacsplus" | 7 | August 25, 2025 |
Scopus | (TITLE-ABS-KEY((propolis OR "Brazilian green propolis") AND (hydrogel OR gel OR thermosensitive OR "temperature-sensitive" OR thermoresponsive OR mucoadhesive)) AND TITLE-ABS-KEY(periodontitis OR "periodontal disease" OR "periodontal diseases" OR gingivitis)) | 30 | August 25, 2025 |
MEDLINE (PubMed) | (("Propolis"[MeSH Terms] OR "Propolis"[Title/Abstract] OR "Brazilian green propolis"[Title/Abstract]) AND ("Hydrogels"[MeSH Terms] OR "hydrogel"[Title/Abstract] OR "gel"[Title/Abstract] OR "thermosensitive"[Title/Abstract] OR "temperature-sensitive"[Title/Abstract] OR "thermoresponsive"[Title/Abstract] OR "mucoadhesive"[Title/Abstract]) AND ("Periodontitis"[MeSH Terms] OR "Periodontal Diseases"[MeSH Terms] OR "Gingivitis"[MeSH Terms] OR "Periodontitis"[Title/Abstract] OR "periodontal disease"[Title/Abstract] OR "Periodontal Diseases"[Title/Abstract] OR "Gingivitis"[Title/Abstract])) | 17 | August 25, 2025 |
Web of Science | ("propolis" OR "Brazilian green propolis") AND ("hydrogel" OR "gel" OR "thermosensitive" OR "temperature-sensitive" OR thermoresponsive OR mucoadhesive*) AND ("periodontitis" OR "periodontal disease" OR "gingivitis") (All Fields) | 29 | August 25, 2025 |
Results
The studies selected from the databases were imported into the Rayyan manager, where 98 records were initially identified, and 56 remained after duplicate removal. A reviewer selected the studies by reading the titles and abstracts. When uncertainty arose regarding eligibility based on title and abstract, the full text was retrieved for further evaluation. In addition, all studies that appeared potentially eligible based on the abstracts were also assessed in full text. In total, 22 articles were evaluated in full; however, 1 article could not be retrieved. Ultimately, 10 studies were included, and 46 were excluded, as illustrated in Figure 1, adapted from PRISMA 2020 flow diagram (Figure 1)13.
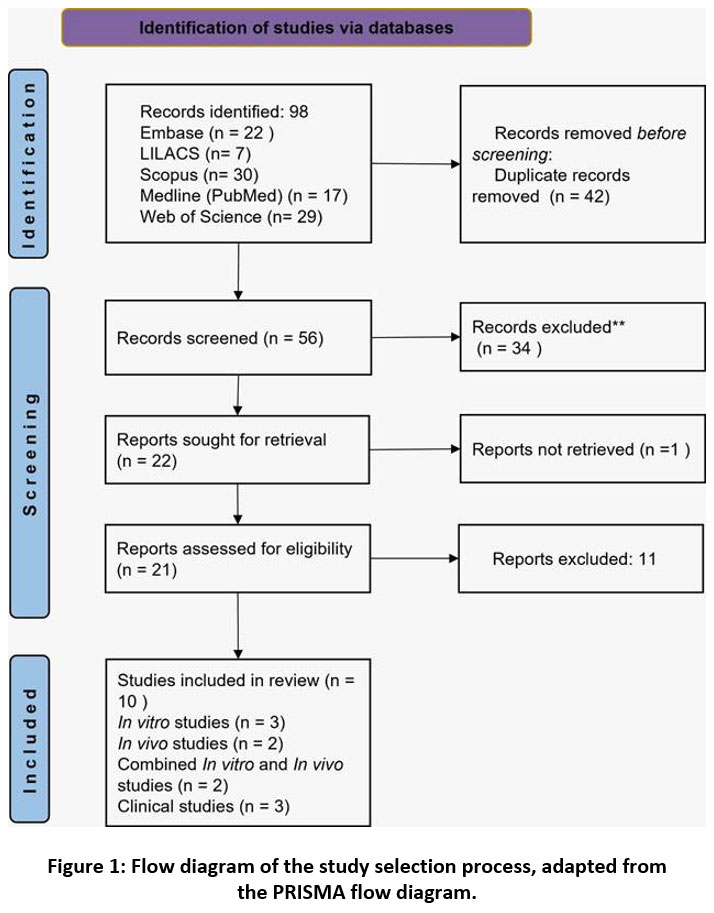 | Figure 1: Flow diagram of the study selection process, adapted from the PRISMA flow diagram.
|
The formulations identified in the included studies comprised:
A thermosensitive cubic liquid crystal hydrogel containing phytosterol triol, total flavonoid extract of propolis, and carbitol11;
Semisolid systems composed of poloxamer 407, carbopol, and 4% propolis extract (PE)14;
A gel containing 35% propolis and dimethyl sulfoxide15;
A gel formulated with Carbopol 940, sodium carboxymethylcellulose (NaCMC) and 10% PE16.
Formulations prepared with stingless bee propolis extract (50%, 60% and 70%), distilled water, triethanolamine, and carbopol17. Another study used a similar composition consisting of propolis extract (at concentrations of 50%, 60%, and 70%), distilled water, triethanolamine, and carbopol.18 The composition of the propolis gel was not reported in some studies19-22.
In vitro studies
Several in vitro studies have investigated the characteristics of gels intended for periodontal application.11,14-17 Rheological analyses showed that the gels exhibited pseudoplastic behavior. In addition, satisfactory viscosity and injectability were reported.11,14-16 The release of propolis components from the polymer matrix was confirmed in multiple studies.11,14,16 All studies reported sustained drug release, with some formulations maintaining drug delivery for more than seven days14,16. Additionally, mucoadhesion was satisfactory for periodontal administration.14-16 Increasing concentrations of propolis extract resulted in reduced gel mucoadhesion, although adhesion remained favorable under periodontal pocket temperature conditions.14
The antimicrobial effectiveness of propolis gels varied. Microorganisms were tested according to the propolis concentration. Higher concentrations were more effective17. However, the antimicrobial activity of propolis-based gels against P. gingivalis has been controversial. While one study showed that propolis gel was not effective against P. gingivalis.16 another study demonstrated inhibitory activity against this microorganism. Furthermore, the 70% propolis extract exhibited greater antimicrobial efficacy against P. gingivalis than 0.2% chlorhexidine.17
In vivo studies
In vivo studies evaluating periodontal parameters reported heterogeneous findings. A thermosensitive hydrogel containing propolis flavonoids decreased the infiltration of inflammatory cells, preserved gingival tissue architecture, and led to a decrease in probing pocket depth (PPD).11 In another, an increased number of fibroblasts, particularly in the group treated with 70% propolis gel, and a decrease in the number of neutrophils were reported.18 In contrast, Soekanto et al. 2021 did not detect significant differences in PPD or alveolar bone loss between animals treated with 5% and 10% propolis gels and the placebo group, which may reflect methodological differences and the short follow-up period.19 Propolis gels were also shown to decrease pro-inflammatory cytokine IL-1 and matrix metalloproteinases such as MMP-2, MMP-8, and MMP-9. In addition, they exhibited anti-inflammatory effects through the inhibition of TLR4/MyD88/NF-?B p65 pathway.11,17
Clinical studies
The efficacy of propolis gels in the treatment of periodontitis and gingivitis was evaluated in three clinical studies20-22, two of which were randomized clinical trials.20-21 None of these studies reported the composition of the propolis hydrogel. Propolis gels have been used both as adjuvants to scaling and root planing (SRP)20 or as components of dental formulations intended for brushing.21-22
The group treated with propolis gel as an adjunct to root planing showed a statistically significant reduction in gingival inflammation (GI). A significant decrease in PI, PPD, and clinical attachment level (CAL) was observed at both 1 and 3 months in all groups. However, the adjunctive use of propolis gel did not result in statistically significant differences when compared with the SRP-only group20. The use of propolis gel in dental formulations for brushing improved the results of PI, GI, PPD, and CAL in patients with periodontitis21. In addition, the bleeding index was lower in the group that used propolis gel in brushing formulations, suggesting a beneficial effect in cases of gingivitis.21-22
Table 2: Propolis gel formulations, administration protocols, and main clinical findings of the included studies
Citation | Type of study | Composition | Form of administration | Conclusion |
Bruschi et al., 200714 | In vitro | Semisolid systems with poloxamer 407, carbopol, and propolis extract 4% | Not reported | Suitable rheological, mechanical, and mucoadhesive properties for periodontal application. |
Aslani et al., 201616 | In vitro | Carbopol 940, (NaCMC), and propolis extract 10% | Not reported | Demonstrated adequate viscosity and mucoadhesive properties, along with an optimal propolis release profile. |
Khaing et al., 202115 | In vitro | Propolis 35 % and dimethyl sulfoxide | Not reported | The in situ forming gel of propolis demonstrated good release and showed an inhibitory effect against three microorganisms (S. aureus, C. albicans, and S. mutans), but no activity against P. gingivalis and E. coli. |
Soekanto et al., 202119 | In vivo | Not reported | Subgingival administration | The 5% and 10% propolis gels exhibited no significant therapeutic effect on periodontitis in a Mus musculus experimental model. |
Maharani et al., 202418 | In vivo | Propolis extract (50%, 60%, and 70%), distilled water, triethanolamine and carbopol | Subgingival administration + SRP | The 70% propolis extract gel showed the highest effectiveness in accelerating periodontal healing, suggesting its potential as an adjunctive therapy for periodontitis. |
Tang et al., 202411 | In vitro and in vivo | Cubic liquid crystal hydrogel with phytosterol triol, total flavonoid extract of propolis and carbitol | Subgingival administration | Thermosensitive cubic liquid crystal hydrogel deposition achieved multiple periodontal protection, reducing the level of periodontal inflammation, promoting osteogenic differentiation, and periodontal tissue regeneration. |
Wulandari et al., 202417 | In vitro and in vivo | Extract of stingless bee propolis (50%, 60% and 70%), distilled water, triethanolamine and carbopol | Subgingival administration | Propolis is a substance that can be used as an adjunctive therapy for periodontitis, helping to reduce inflammation and promote the healing process. |
Tanasiewicz et al., 201222 | Clinical study | Not reported | Dental formulations for brushing | Propolis gel showed an anti-inflammatory effect on the gingival tissues. |
Kumar et al., 201521 | Clinical study | Not reported | SRP + Dental formulations for brushing | Propolis gel led to a decrease in red complex microorganisms and a reduction in clinical parameters (PI,GI, Bleeding on Probing, PPD, and CAL). |
Aggarwal et al., 202320 | Clinical study | Not reported | Subgingival administration + SRP | Propolis gel + SRP demonstrated favorable clinical changes within the group itself, but without significant differences compared to conventional treatment (SRP). |
Discussion
Recently, there has been an increasing interest in natural products. Propolis has been studied as an adjunct to periodontal treatment due to its anti-inflammatory, antimicrobial, antioxidant, and immunomodulatory properties. Its incorporation into gel formulations has gained relevance, as these systems allow site-specific action, uniform distribution, and sustained release of the active ingredient23-24.
Physicochemical and Rheological Properties
The study of rheological properties is essential for gel formulations, since characteristics such as spreadability, syringability, and texture determine their clinical applicability25. The in vitro studies included in this review showed that propolis gels exhibited adequate viscosity and injectability, as well as mucoadhesion properties and controlled release of the active ingredient11, 14-17. However, heterogeneity in composition was observed, a factor that directly impacts physicochemical properties. Carbopol was the most frequently used polymer14, 16-18, and higher concentrations were associated with greater hardness, compressibility, and mucoadhesion, but with reduced drug release, findings consistent with Alfaris et al. 202226. Similarly, the literature describes that higher concentrations of poloxamer are also related to increased mucoadhesion27.
In addition to the basic elements required for gel formulation, the incorporation of propolis also influenced the physicochemical properties of the gels, particularly mucoadhesion. Mucoadhesion refers to the ability of a formulation to adhere to the mucosal epithelium and for maintaining the product at the target site28. Its occurrence depends on the expansion of polymer chains, with the formation of hydrogen bonds between the hydrophilic groups of the polymer and the mucin present in the mucosa16. In this context, one study reported that increasing propolis concentrations reduced mucoadhesive strength14, contrary to the findings of Khaing et al., 2021, who found an increase in mucoadhesion with the incorporation of propolis, in agreement with Berreta et al., 201315,25. These authors demonstrated that propolis incorporation increased mucoadhesion in carbopol and poloxamer gels, whereas no significant effect was observed in alginate and chitosan-based hydrogels25. Propolis also increased gel viscosity15, corroborating previous findings29, and modified the pseudoplastic profile in chitosan and poloxamer gels, but not carbopol formulations.25. Therefore, these results indicate that the influence of propolis incorporation on mucoadhesion and rheological properties may vary according to the polymers used in the formulation of the gels and the concentration of propolis.
Gels for periodontal administration should provide controlled and sustained drug release. For greater reliability, the evaluation of propolis component release should be performed under conditions that simulate the periodontal environment (temperature, pH, presence of gingival crevicular fluid)14. Despite methodological heterogeneity, all studies consistently demonstrated effective release of propolis components from the polymer matrix, supporting the feasibility of these systems for controlled periodontal delivery11,14-16. Regarding the pH of propolis gels, values ranged between 5 and 6, whereas the pH of propolis extract itself was slightly higher, between 6 and 7. The pH values of the propolis gels were considered adequate for periodontal administration, as they did not cause irritation and were close to the ideal pH of the periodontal pocket, approximately 6.216.
In Vitro Antimicrobial Activity
The antimicrobial activity of propolis gels varied across studies. Formulations at 35% were effective against S. aureus, C. albicans, and S. mutans, but not against P. gingivalis, while in other studies propolis in concentrations of 10% and 70% demonstrated activity against this periodontal pathogen16-17. Agarwal et al. 2012 reinforce the potential of chinese propolis by demonstrating activity against P. gingivalis and A. actinomycetemcomitans30. These differences may be attributed to variations in the chemical composition and concentration of bioactive compounds among different types of propolis that may influence antimicrobial efficacy. That suggest that propolis may exhibit in vitro antimicrobial activity against periodontal pathogens, depending on its composition and concentration. Therefore, it could be considered a potential natural adjunct to periodontal therapy. This approach may contribute to reducing reliance on antibiotics and chlorhexidine, whose antimicrobial efficacy is well established but accompanied by cytotoxicity, even in gel formulations5,30. Nevertheless, concentrations of propolis extract that are effective against periodontal pathogens have also been associated with cytotoxicity in gingival fibroblasts, in an apparently dose-dependent manner31-32. It is important to highlight that the cytotoxicity of propolis gels was not evaluated in the studies included in this review, representing a gap that should be addressed in future investigations.
Anti-Inflammatory, Immunomodulatory, and Regenerative Effects
Studies have shown that propolis reduces the release of pro-inflammatory cytokines, the transcription factor NF-?B, and NLRP inflammasomes, in addition to suppressing signaling pathways associated with the inflammatory response33. Similarly, propolis gels have demonstrated relevant anti-inflammatory and regenerative effects in in vivo models. In these investigations, hydrogels were able to reduce the number of inflammatory cells and IL-1? levels, and suppressed the expression of TLR4 (Toll-like receptors)/MyD88/NF-?B p65, an innate immunity signaling pathway involved in the activation of pro-inflammatory mediators and the induction of apoptosis. A decrease in reactive oxygen species was also observed in animals treated with propolis hydrogel, further reinforcing its antioxidant properties11.
The reduction in the expression of matrix metalloproteinases (MMPs), including MMP2 and MMP-9, RANKL, and the number of osteoclasts, factors associated with collagen degradation and bone resorption, combined with an increase in RUNX-2 and ALP, proteins associated with osteoblastic activity, demonstrates the protective potential of propolis gels on periodontal tissues. This effect was confirmed by microtomography in the study by Tang et al. 2024, which also attributed regenerative properties in the periodontium in vivo to propolis flavonoid gel11. Other studies have associated propolis with increased collagen deposition, enhanced angiogenesis, re-epithelialization, and reduced fibrosis, results achieved through decreased release of histamine and pro-inflammatory cytokines, as well as a reduction in the number of mast cells33. However, these findings are derived from animal models, and direct extrapolation to clinical periodontal therapy should be interpreted with caution.
Therapeutic Effects on Periodontal Parameters in Animal Models
Regarding PPD in vivo, Tang et al., 2024 reported a reduction in this parameter in the groups treated with the hydrogel containing propolis flavonoids11. Although in vivo studies highlight the therapeutic potential of propolis in the treatment of periodontal disease, there are still inconsistent results. Soekanto et al. 2021 reported that 5% and 10% propolis gels did not have a significant therapeutic effect in the treatment of periodontitis, as no differences in PPD or alveolar bone loss were observed between the propolis-treated groups and the control group19. However, it is important to note that the study had a short duration, lasting only 14 days, which may have limited the extent of bone loss observed. In addition, this parameter was evaluated in a restricted manner, as bone loss was quantified in only two dimensions. It should also be considered that the authors did not perform mechanical therapy to control periodontal disease, a factor that may have further limited the observed therapeutic effects. However, Tang et al., 2024 did not use scaling and root planing and were still able to demonstrate favorable results with the application of propolis gel, suggesting that the absence of conventional therapy is not the only determining factor11. Furthermore, these differences may be related both to the different animal species used—such as Wistar rats, Sprague-Dawley rats, and Mus musculus mice—and to the different experimental models employed to induce periodontitis. It is known that the response to the periodontal inflammatory process may vary according to the animal strain and the method used to induce the disease, whether by ligature alone or in association with P. gingivalis inoculation. In this context, pathogen inoculation has been described as a factor that exacerbates periodontal destruction, intensifying inflammatory responses and accelerating tissue breakdown34.
Therapeutic Effects on Periodontal Parameters in Clinical Studies
In the clinical studies evaluated, improvements in periodontal parameters associated with the use of propolis were observed, either as an adjunct gel to scaling and root planing or as a gel applied during brushing after SRP. Regarding PPD and CAL, two studies reported clinically favorable reductions; however, in the trial that investigated propolis gel in combination with conventional mechanical therapy, these improvements did not differ statistically from those achieved with basic periodontal treatment alone, suggesting no additional benefit from combining adjunctive therapy20. It is important to consider that the intragroup improvements observed in the clinical parameters may be primarily attributed to periodontal instrumentation rather than to the effect of the propolis gel itself. On the other hand, the study that evaluated the gel applied during toothbrushing demonstrated significant improvements in these same outcomes, suggesting a potential contribution of propolis when incorporated into the daily oral hygiene routine21-22. However, it should be noted that, in one of the studies, the use of brushing gels was combined with scaling and root planing, which may also have influenced the results21.
Regarding inflammatory outcomes, two studies that used propolis gel for brushing reported reduced gingival bleeding and improvements in gingivitis, reinforcing the anti-inflammatory potential of the substance21-22. In the study by Tanasiewicz et al., 2012, this parameter was significant only in the group that exhibited adequate oral hygiene, with no alterations in the marginal periodontium22. However, although the adjunctive gel group showed intragroup improvements in GI and PI after SRP, these changes were not statistically different from those observed in the control group, indicating no additional benefit of propolis beyond mechanical therapy alone20.
Overall Considerations, Limitations, and Future Perspectives
It is important to consider that the composition of propolis may vary according to its botanical origin and geographical location, which directly influences its bioactivity profile30. Moreover, differences in the concentrations used and heterogeneity in gel formulations across studies may explain some of the discrepancies observed in the results. It should be noted, however, that none of the clinical studies reviewed provided a detailed description of the composition of the propolis gel used, which limits reproducibility and hinders the identification of the components responsible for the observed effects. In addition, the samples were small and follow-up periods were short, factors that restrict the generalization of the findings. Taken together, the available evidence supports the beneficial effects of propolis in the control of periodontal diseases, but also reinforces the need for clinical trials with larger sample sizes, standardized formulation descriptions, and long-term follow-up to confirm its efficacy and safety. The clinical studies evaluated suggest that gels containing propolis have therapeutic potential in controlling periodontal clinical parameters; however, these effects should be interpreted with caution, as the studies employed different methodologies and present several limitations.
Conclusion
The findings indicate that the propolis gels exhibit physical properties suitable for periodontal disease management, including appropriate viscosity, injectability, mucoadhesion, and sustained release profile. In vivo findings suggest a promising adjunctive role in the management of periodontitis and gingivitis. However, additional clinical trials are needed to confirm their efficacy and safety in the treatment of periodontal diseases.
Acknowledgement
The authors thank the National Council for Scientific and Technological Development (CNPq) for scholarship 304606/2021-9 to M.T.J., Coordination for the Improvement of Higher Education Personnel (CAPES) (Finance Code 001), and Dr. Emanuela Prado Ferraz for assistance during manuscript preparation.
Funding Sources
This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Brasil (CAPES) – Finance Code 001 and the National Council for Scientific and Technological Development (CNPq) grant number 304606/2021-9 to M.T.J.
Conflict of Interest
The authors do not have any conflict of interest.
Data Availability Statement
This statement does not apply to this article.
Ethics Statement
This research did not involve human participants, animal subjects, or any material that requires ethical approval.
Informed Consent Statement
This study did not involve human participants, and therefore, informed consent was not required.
Clinical Trial Registration
This research does not involve any clinical trials.
Permission to Reproduce Material from other Sources
Not applicable.
Authors’ Contribution
Ana Carolina Duarte Firmino: Conceptualization, literature search, article selection, data extraction, writing – original draft.
Nathalya Maria Vileila Moura: Writing – review & editing.
Mario Taba Jr.: Writing – review & editing, supervision.
Reference
- Hajishengallis G. Interconnection of periodontal disease and comorbidities: evidence, mechanisms, and implications. Periodontol 2000. 2022;89(1):9-18.
CrossRef - Loos BG, Van Dyke TE. The role of inflammation and genetics in periodontal disease. Periodontol 2000. 2020;83(1):26-39.
CrossRef - Sanz M, Herrera D, Kebschull M, et al. Treatment of stage I–III periodontitis: the EFP S3 level clinical practice guideline. J Clin Periodontol. 2020;47(Suppl 22):4-60.
CrossRef - Pezzella V, Cuozzo A, Mauriello L, et al. Propolis as an adjunct in non-surgical periodontal therapy: current clinical perspectives from a narrative review. J Funct Biomater. 2025;16(7):265.
CrossRef - Gegout PY, Stutz C, Huck O. Gels as adjuvant to non-surgical periodontal therapy: a systematic review and meta-analysis. Heliyon. 2023;9(7):e17789.
CrossRef - Chen Y, Wang X, Tao S, et al. Research advances in smart responsive-hydrogel dressings with potential clinical diabetic wound healing properties. Mil Med Res. 2023;10(1):37.
CrossRef - Garg A, Agrawal R, Singh Chauhan C, Deshmukh R. In-situ gel: a smart carrier for drug delivery. Int J Pharm. 2024;652:123819.
CrossRef - López-Valverde N, Pardal-Peláez B, López-Valverde A, et al. Effectiveness of propolis in the treatment of periodontal disease: updated systematic review with meta-analysis. Antioxidants (Basel). 2021;10(2):269.
CrossRef - Zulhendri F, Lesmana R, Tandean S, et al. Recent update on the anti-inflammatory activities of propolis. Molecules. 2022;27(23):8473.
CrossRef - Bava R, Puteo C, Lombardi R, et al. Antimicrobial properties of hive products and their potential applications in human and veterinary medicine. Antibiotics (Basel). 2025;14(2):172.
CrossRef - Tang M, Li J, Wang G, et al. Cubic liquid crystals containing propolis flavonoids as in situ thermo-sensitive hydrogel depots for periodontitis treatment: preparation, pharmacodynamics and therapeutic mechanisms. Eur J Pharm Sci. 2024;196:106762
CrossRef. - Assunção M, Carneiro VMA, Stefani CM, de Lima CL. Clinical efficacy of subgingivally delivered propolis as an adjuvant to nonsurgical periodontal treatment of periodontitis: a systematic review and meta-analysis. Phytother Res. 2021;35(10):5584-5595.
CrossRef - Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71.
CrossRef - Bruschi ML, Jones DS, Panzeri H, et al. Semisolid systems containing propolis for the treatment of periodontal disease: in vitro release kinetics, syringeability, rheological, textural, and mucoadhesive properties. J Pharm Sci. 2007;96(8):2074-2089.
CrossRef - Khaing EM, Intaraphairot T, Chuenbarn T, et al. Natural resin-based solvent exchange induced in-situ forming gel for vancomycin HCl delivery to periodontal pocket. Mater Today Proc. 2021;47:3585-3593.
CrossRef - Aslani A, Malekpour N. Design, formulation, and physicochemical evaluation of periodontal propolis mucoadhesive gel. Dent Res J (Isfahan). 2016;13(6):484-493.
CrossRef - Wulandari P, Zulhendri F, Hanafiah OA, et al. Phytochemical analysis and effectiveness of stingless bees propolis (Geniotrigona thoracica) on matrix metalloproteinase-8 levels in periodontal therapy. Int J Appl Pharm. 2024;16(Suppl 2):22-28.
CrossRef - Maharani J, Dalimunthe A, Wulandari P, et al. Effectiveness of propolis extract gel as adjunctive periodontal therapy: overview of fibroblasts and neutrophils (in vivo study). Int J Appl Pharm. 2024;16(2):15-21.
CrossRef - Soekanto SA, Safitri YN, Zeid H, et al. Effectiveness of propolis gel on Mus musculus (Swiss Webster) periodontitis model with ligature silk thread application. AIP Conf Proc. 2021;2344:040008.
CrossRef - Aggarwal R, Bawa SS, Palwankar P, et al. To evaluate the clinical efficacy of 940 nm diode laser and propolis gel as adjunct to scaling and root planing in treatment of chronic periodontitis. J Pharm Bioallied Sci. 2023;15(Suppl 2):S1218-S1220.
CrossRef - Kumar A, Sunkara MSVV, Pantareddy I, Sudhakar S. Comparison of plaque inhibiting efficacies of Aloe vera and propolis tooth gels: a randomized PCR study. J Clin Diagn Res. 2015;9(9):ZC01-ZC03.
CrossRef - Tanasiewicz M, Skucha-Nowak M, Dawiec M, et al. Influence of hygienic preparations with a 3% content of ethanol extract of Brazilian propolis on the state of the oral cavity. Adv Clin Exp Med. 2012;21(1):81-92.
- El-Nablaway M, Rashed F, Taher ES, et al. Bioactive injectable mucoadhesive thermosensitive natural polymeric hydrogels for oral bone and periodontal regeneration. Front Bioeng Biotechnol. 2024;12:1384326.
CrossRef - Rajendran S, Kumar KS, Ramesh S, Rao SR. Thermoreversible in situ gel for subgingival delivery of simvastatin for treatment of periodontal disease. Int J Pharm Investig. 2017;7(2):101-106.
CrossRef - Berretta AA, de Castro PA, Cavalheiro AH, et al. Evaluation of Mucoadhesive Gels with Propolis (EPP-AF) in Preclinical Treatment of Candidiasis Vulvovaginal Infection. Evid Based Complement Alternat Med. 2013;2013:641480.
CrossRef - Alfaris SM, Dhahir RK, Al-Nima AM. Preparation, evaluation of propolis extract gel and exploring its antioxidant and antimicrobial activity. Pharmacogn J. 2022;14(6):675-681.
CrossRef - Pereira RR, Ribeiro-Godoy JS, Stivalet-Svidzinski TI, Bruschi ML. Preparation and characterization of mucoadhesive thermoresponsive systems containing propolis for the treatment of vulvovaginal candidiasis. J Pharm Sci. 2013;102(4):1222-1234.
CrossRef - Okur NÜ, Bülbül EÖ, Ya?c?lar AP, Siafaka PI. Current status of mucoadhesive gel systems for buccal drug delivery. Curr Pharm Des. 2021;27(17):2015-2025.
CrossRef - Ferreira LMMC, Modesto YY, Souza PDQ, et al. Characterization, biocompatibility and antioxidant activity of hydrogels containing propolis extract as an alternative treatment in wound healing. Pharmaceuticals (Basel). 2024;17(5):575.
CrossRef - Agarwal G, Vemanaradhya GG, Mehta DS. Evaluation of chemical composition and efficacy of Chinese propolis extract on Porphyromonas gingivalis and Aggregatibacter actinomycetemcomitans: an in vitro study. Contemp Clin Dent. 2012;3(3):256-261.
CrossRef - Sonmez S, Kirilmaz L, Yucesoy M, et al. The effect of bee propolis on oral pathogens and human gingival fibroblasts. J Ethnopharmacol. 2005;102(3):371-376.
CrossRef - Millones-Gómez PA, De la Garza-Ramos MA, Urrutia-Baca VH, et al. Cytotoxicity of Peruvian propolis and Psidium guajava on human gingival fibroblasts, PBMCs and HeLa cells. F1000Res. 2022;11:430.
CrossRef - Loya-Hernández LP, Arzate-Quintana C, Castillo-González AR, et al. Propolis-functionalized biomaterials for wound healing: a systematic review with emphasis on polysaccharide-based platforms. Polysaccharides. 2025;6(3):74.
CrossRef - Struillou X, Boutigny H, Soueidan A, Layrolle P. Experimental animal models in periodontology: a review. Open Dent J. 2010;4:37-47.
CrossRef
Abbreviations List
APT – adjunctive periodontal therapy
ATP – adenosine triphosphate
CAPE – caffeic acid phenyl ester
COX – cyclooxygenase
GI – gingival inflammation
LOX – lipoxygenase
MMP – matrix metalloproteinase
NaCMC – sodium carboxymethylcellulose
NSPT – non-surgical periodontal treatment
PD – periodontal disease
PE – propolis extract
PPD – probing pocket depth
SRP – scaling and root planing





