.jpg)
Rehabilitation of an Atrophic Maxilla using the All-On-Four Protocol: A Case Report
Marília Soares1  , Vivian Eduarda1 , Thiago Bartko1 , Paula Spinelli1 , Leandro Lécio de Lima Sousa1 , Sergio Charifker Ribeiro Martins1 and Gustavo Vicentis Oliveira Fernandes2*
, Vivian Eduarda1 , Thiago Bartko1 , Paula Spinelli1 , Leandro Lécio de Lima Sousa1 , Sergio Charifker Ribeiro Martins1 and Gustavo Vicentis Oliveira Fernandes2*
1Department of Implantology and Prosthodontics, FUNORTE - Faculdades Integradas do Norte de Minas, Recife/PE, Brazil .
2A.T. Still University – Missouri School of Dentistry and Oral Health, St. Louis, MO, U.S.A .
http://dx.doi.org/10.12944/EDJ.07.0102.07
Oral rehabilitation of the atrophic maxilla is a common clinical challenge, especially in edentulous patients, due to significant bone loss that compromises implant stability and smile esthetics. The All-on-Four protocol has emerged as an effective, minimally invasive, and predictable alternative, eliminating the need for bone grafting procedures while promoting satisfactory functional and aesthetic outcomes. This case report presents a clinical scenario of the rehabilitation of an atrophic maxilla using the All-on-Four technique. The patient, a 70-year-old female who was fully edentulous in the maxilla, reported aesthetic and functional dissatisfaction with her current prosthesis. After clinical and tomographic evaluation, the All-on-Four protocol was indicated for the placement of four Morse taper implants. Two anterior straight implants and two posterior implants angled at 45° were placed to maximize bone utilization and avoid the maxillary sinus. The surgical procedure was performed under local anesthesia, followed by relining of the provisional prosthesis. No adverse event or complications were observed on the day of the surgical procedure or in the postoperative period. After the osseointegration period, intermediate abutments were placed, and the definitive prosthesis was installed. After 6 months, the patient reported complete satisfaction with the treatment, which enhanced both the esthetic and masticatory functions. The case report demonstrates the benefits of the technique, including reduced treatment time, good primary stability, absence of significant morbidity, and excellent functional and esthetic outcomes for the patient. The All-on-Four protocol proved to be an effective and safe rehabilitative solution for cases of atrophic maxilla, contributing to improvements in the patient’s quality of life.
Copy the following to cite this article:
Soares M, Eduarda V, Bartko T, Spinelli P, Sousa L. L. D. L, Martins S. C. R, Fernandes G. V. O. Rehabilitation of an Atrophic Maxilla using the All-On-Four protocol: A Case Report. Enviro Dental Journal 2025; 7(1).
DOI:http://dx.doi.org/10.12944/EDJ.07.0102.07Copy the following to cite this URL:
Soares M, Eduarda V, Bartko T, Spinelli P, Sousa L. L. D. L, Martins S. C. R, Fernandes G. V. O. Rehabilitation of an Atrophic Maxilla using the All-On-Four protocol: A Case Report. Enviro Dental Journal 2025; 7(1).Available here:https://bit.ly/4nts8cE
.
Download article (pdf) Citation Manager

Introduction
Tooth loss is a condition that entails significant functional and social consequences for edentulous individuals, directly compromising masticatory capacity, phonetics, esthetics, and nutritional status. In more complex cases, it may also affect self-esteem, negatively impacting patients’ social life.1 With the increase in life expectancy observed in most countries, tooth loss and alveolar bone resorption have become increasingly common conditions.2,3 Edentulism affects all social classes and reflects both living conditions and the availability of healthcare services for the population. In this context, dental specialties continuously seek alternatives to promote the oral rehabilitation of patients with tooth loss.1
The process of bone resorption is complex and may involve horizontal and/or vertical resorption of the alveolar crest, as well as maxillary sinus pneumatization. These factors reduce the available bone height for implant placement, often necessitating a sinus augmentation procedure to increase bone volume4 and enable the proper selection of implant length. Such procedures inevitably add time, morbidity, and treatment cost.
Given the need to restore masticatory function, esthetics, and phonetics, several techniques have been developed over the years. A promising alternative in this context, and the focus of the present study, is the All-on-Four technique, which stands out for its predictability and efficiency in treatment.2,3,5
The All-on-Four clinical approach consists of placing four anterior implants to support a prosthesis in edentulous patients. The two posterior implants are distally inclined at an angle of 35° to 45°, which allows the use of longer implants and enhances primary stability, thereby eliminating – in most cases – the need for sinus augmentation.6 This technique offers several advantages, including greater prosthesis stability with reduced cantilever, elimination of the need for bone grafting, lower treatment costs, ease of maintenance, reduced morbidity, shorter treatment times, and significant improvements in quality of life.6
Currently, multiple options are available for oral rehabilitation in edentulous patients,7-9 with conventional removable dentures still widely used due to their lower cost. However, this treatment modality presents several functional and esthetic limitations and fails to prevent progressive bone resorption, often leading to problems with retention and adaptation. With advances in implant dentistry, implants and implant-supported prostheses have emerged as a superior alternative, preventing further resorption and being regarded as the gold standard for oral rehabilitation.1,10
This case report aimed to present a clinical case of full maxillary rehabilitation in an atrophic maxilla, where the treatment of choice was oral rehabilitation using the All-on-Four protocol.
Materials and Methods
The patient, D.M.S., a 70-year-old melanodermic female, classified as ASA II, presented with complete edentulism in the maxilla and partial edentulism in the mandible. She reported wearing a total maxillary denture for more than 10 years (Figure 1), which exhibited poor esthetics and function, and required additional retention with denture adhesives. Her chief complaint was dissatisfaction with her smile. The patient signed an informed consent prior to start of the clinical treatment.
 | Figure 1: Initial frontal image with a complete maxillary denture. |
The clinical examination revealed loss of upper lip support, decreased vertical dimension of occlusion, unsatisfactory overbite, and unfavorable esthetics of the existing prosthesis (Figure 2). Additionally, the maxilla showed significant atrophy, as indicated by reduced bone height and buccolingual width (Figure 3).
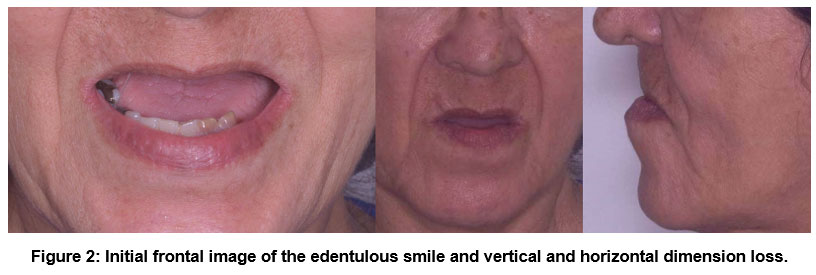 | Figure 2: Initial frontal image of the edentulous smile and vertical and horizontal dimension loss. |
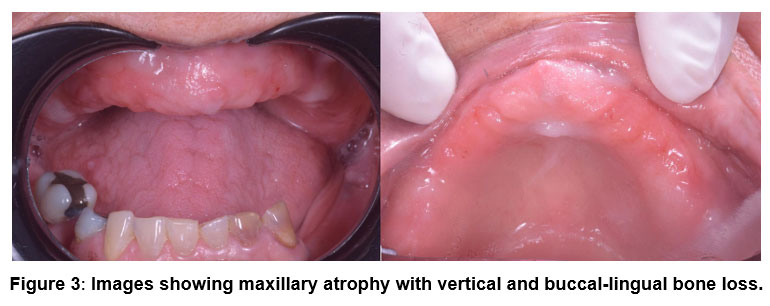 | Figure 3: Images showing maxillary atrophy with vertical and buccal-lingual bone loss. |
Laboratory tests and cone-beam computed tomography (CBCT) were requested for assessment and surgical treatment planning. Based on the clinical and radiographic findings, the treatment plan consisted of placing four implants using the All-on-Four protocol, thereby avoiding sinus augmentation surgery and the use of extra-short implants.
Results
The surgical phase was performed under local anesthesia with vasoconstrictor (articaine 1:200,000). A supracrestal linear incision with posterior releasing incisions was made to allow full-thickness flap elevation. Sequential drilling was performed for Morse-taper implants using the corresponding system-specific burs. Four Morse-taper implants (Titanium Fix B-Fix, Brazil) were placed: two anterior implants measuring 4.0 × 8.5 mm and two posterior implants measuring 4.0 × 15 mm. The posterior implants were installed at angulations of 30° and 45° angulation, respectively (Figure 4). All implants achieved a final insertion torque of 45 N·cm. Healing abutments were placed, and the surgical site was sutured with 5-0 nylon, leaving the implants submerged. The existing prosthesis was relined with soft acrylic resin and used as a provisional prosthesis without immediate loading. No adverse events were observed.
Three months after surgery, a panoramic radiograph was obtained (Figure 4) to evaluate bone healing and implant positioning. A reentry surgery was performed, and the following multi-unit abutments were installed: anterior straight abutments (left transmucosal height: 4 mm; right: 3 mm) and posterior angulated abutments (left: 30° and 3.5 mm transmucosal height; right: 17° and 2.5 mm transmucosal height) (Figure 5).
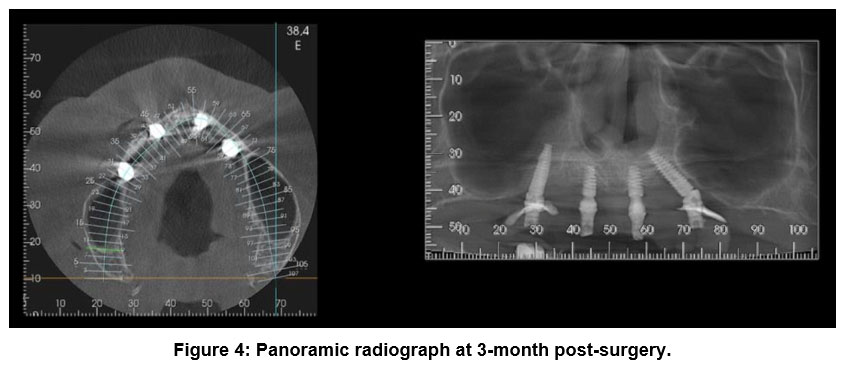 | Figure 4: Panoramic radiograph at 3-month post-surgery. |
 | Figure 5: Implant position with the intermediate abutment. |
The prosthesis pickup was performed using metallic copings (Figure 6). The prosthesis was prepared (Figure 5) for capture with autopolymerizing acrylic resin and subsequently installed (Figure 7). The prosthesis was designed with a convex intaglio surface to facilitate hygiene and maintain peri-implant health. An immediate improvement in the patient’s facial profile was observed (Figure 8). The patient expressed immediate satisfaction with the rehabilitation; after 6 months, the patient confirmed complete satisfaction with the treatment, which enhanced both the esthetic and masticatory functions.
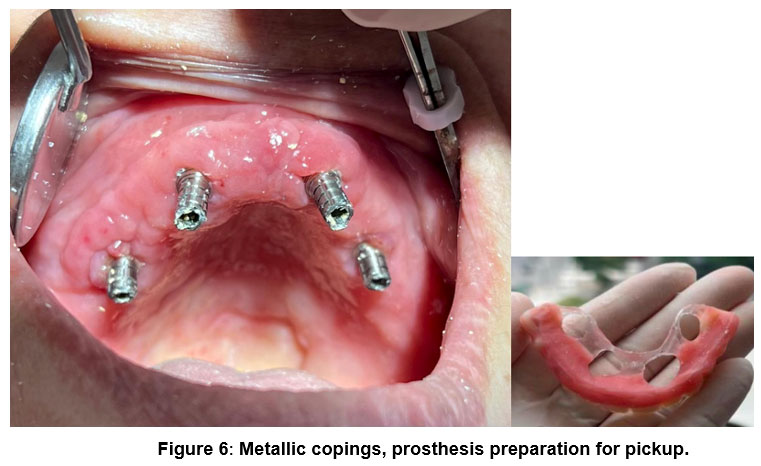 | Figure 6: Metallic copings, prosthesis preparation for pickup. |
 | Figure 7: Installation of the definitive maxillary fixed prosthesis (All-on-Four protocol). |
 | Figure 8. An immediate profile showing the recovery of vertical and horizontal dimensions. |
Discussion
Rehabilitation of the atrophic maxilla is a routine condition in dental practice;11-13 however, it continues to pose a challenge for clinicians due to its complexity and the variety of therapeutic approaches available. To reduce the unpredictability of rehabilitative treatment, several criteria must be considered, including accurate diagnosis, a well-structured treatment plan, esthetic and occlusal aspects, the type of prosthesis indicated, and tomographic assessment. Reverse planning and the use of surgical guides are crucial tools in thorough diagnostic analysis, as they help prevent unfavorable implant positioning that could compromise the success of rehabilitation.1
In the presented clinical case, the All-on-Four technique was chosen due to insufficient bone volume in the posterior maxilla, combined with the patient’s desire for a shorter treatment duration, lower surgical morbidity, and improved aesthetic and functional outcomes. Initially, a rehabilitation with a greater number of implants using extra-short implants (reduced length)14-16 was considered; however, the patient opted for the All-on-Four technique. would be beneficial; therefore, the patient opted for the All-on-Four technique. This technique enables the placement of four implants in the maxilla, with two angled distally. Such angulation enables the use of longer implants, optimizes the available bone, and avoids critical anatomical structures, such as the maxillary sinus, thus eliminating the need for bone grafting.6,17,18
The All-on-Four protocol requires a thorough evaluation of the patient’s anatomical conditions to ensure successful osseointegration. A minimum bone height of 10 mm in the anterior region and a thickness of at least 5 mm are essential prerequisites. Additionally, the location of the anterior wall of the maxillary sinus determines the positioning of the posterior implants. In this case, the implants measured 4.0 × 8.5 mm and were positioned 2 mm below the alveolar crest (anterior implants), fully utilizing the available height. By tracing an imaginary line at 45° from the midline, tangent to the sinus wall, the intersection with the alveolar ridge defines the ideal site for posterior implant placement, which was applied in this case.5,19 This technique uses distal implant angulation to enable a full-arch restoration while being less invasive. In the present case, however, a shortened dental arch rehabilitation was planned, with the prosthesis extending only to the first molar (first molar occlusion), since the antagonist arch lacked second and third molars. Posterior angulation reduces the cantilever length, increases the interimplant distance, and facilitates prosthesis maintenance and hygiene.6 The preference for the All-on-Four technique lies in maximizing the use of available bone in atrophic maxillae, thereby avoiding complex regenerative procedures12 that would increase morbidity.20
Despite its advantages, the All-on-Four procedure poses challenges, particularly for less experienced clinicians. The surgery may involve the extraction of compromised teeth, bone leveling, and precise implant insertion. In this case, bone leveling was performed to standardize ridge height, allowing for ideal implant positioning and adaptation of a PF3-type prosthesis selected for rehabilitation. In atrophic maxillae, the proximity of critical anatomical structures and the limited bone availability make the procedure even more complex, especially for posterior implant placement. One strategy that may facilitate the technique is the use of digitally planned surgical guides,8 which guide the surgeon’s movements during implant insertion to ensure optimal positioning according to reverse planning.6 However, in the present case, surgery was performed without the aid of guides, relying solely on radiographic and tomographic parameters and the clinical experience of the surgeon (freehand procedure).
The All-on-Four approach has emerged as an effective alternative to maxillary sinus grafting, providing stable support for dental prostheses and contributing to the preservation of the remaining bone. Its advantages – rapid recovery, reduced postoperative discomfort, and lower cost – reinforce its role as a contemporary and efficient solution for oral rehabilitation.5,20 In this case report, the patient presented no pain postoperatively, experiencing only facial edema without associated symptoms or other adverse outcomes.
Current evidence supports the safety of the All-on-Four technique in restoring masticatory function and esthetics in fully edentulous patients, as confirmed by the clinical case reported herein.1,6
Conclusion
The rehabilitation of the atrophic maxillae presents a significant clinical challenge, requiring careful planning and technical expertise from the dentist. In this context, the All-on-Four protocol stands out as a predictable, effective, and less invasive alternative, providing patients with faster recovery, reduced surgical morbidity, and satisfactory functional and esthetic restoration. Despite the technical requirements involved, the use of digital planning tools significantly contributes to the safety and success of the procedure. The clinical case presented clearly illustrates the benefits of this approach, reinforcing its applicability and effectiveness in the oral rehabilitation of patients with maxillary bone atrophy.
Acknowledgment
I would like to thank of FUNORTE -Faculdades Integradas do Norte de Minas, Recife/PE, Brazil.
Funding Sources
The author(s) received no financial support for the research
Conflict of Interest
The authors do not have any conflict of interest.
Data Availability Statement
This statement does not apply to this article.
Ethics Statement
This article is not a research study; ethical approval is not necessary.
Informed Consent Statement
The patient signed the informed consent prior to the development of the clinical case.
Clinical Trial Registration
This research does not involve any clinical trials.
Permission to reproduce material from other sources
Not applied.
Author Contributions
Conceptualization: Marília Soares, Vivian Eduarda, Thiago Bartko, Paula Spinelli, Leandro Lécio de Lima Sousa;
Methodology: Marília Soares, Vivian Eduarda, Thiago Bartko, Paula Spinelli, Leandro Lécio de Lima Sousa, Sergio Charifker Ribeiro Martins, Gustavo Vicentis Oliveira Fernandes;
Software: Marília Soares, Vivian Eduarda, Leandro Lécio de Lima Sousa, Sergio Charifker Ribeiro Martins, Gustavo Vicentis Oliveira Fernandes;
Validation: Marília Soares, Vivian Eduarda, Thiago Bartko, Paula Spinelli, Leandro Lécio de Lima Sousa, Sergio Charifker Ribeiro Martins, Gustavo Vicentis Oliveira Fernandes;
Formal analysis, Marília Soares, Vivian Eduarda, Thiago Bartko, Paula Spinelli, Leandro Lécio de Lima Sousa, Sergio Charifker Ribeiro Martins, Gustavo Vicentis Oliveira Fernandes;
Investigation, Marília Soares, Vivian Eduarda, Thiago Bartko, Paula Spinelli, Leandro Lécio de Lima Sousa, Sergio Charifker Ribeiro Martins, Gustavo Vicentis Oliveira Fernandes;
Resources, Leandro Lécio de Lima Sousa, Sergio Charifker Ribeiro Martins, Gustavo Vicentis Oliveira Fernandes;
Data curation, MS, Vivian Eduarda, Thiago Bartko, Paula Spinelli, Leandro Lécio de Lima Sousa, Sergio Charifker Ribeiro Martins, Gustavo Vicentis Oliveira Fernandes;
Writing—original draft preparation, Marília Soares, Vivian Eduarda, Thiago Bartko, Paula Spinelli,Leandro Lécio de Lima Sousa, Sergio Charifker Ribeiro Martins, Gustavo Vicentis Oliveira Fernandes;
Writing—review and editing, Marília Soares, Vivian Eduarda, Thiago Bartko, Paula Spinelli, Leandro Lécio de Lima Sousa, Sergio Charifker Ribeiro Martins, Gustavo Vicentis Oliveira Fernandes;
Visualization, Marília Soares, Vivian Eduarda, Thiago Bartko, Paula Spinelli, Leandro Lécio de Lima Sousa, Sergio Charifker Ribeiro Martins, Gustavo Vicentis Oliveira Fernandes;
Supervision, Leandro Lécio de Lima Sousa, Sergio Charifker Ribeiro Martins, Gustavo Vicentis Oliveira Fernandes;
Project administration, Leandro Lécio de Lima Sousa, Sergio Charifker Ribeiro Martins, Gustavo Vicentis Oliveira Fernandes;
References
- Moreira T. C. A., Costa S.L., SILVA Jr E. V., Quidute L. T. C., Cravinhos J. C. P., Firmiano C. S. C., Valente V. S. Reabilitação com implantes em maxila atrófica por meio de cirurgia guiada utilizando a técnica “All-on-four”. Res Soc Developm. 2023;12(5):e27512541725. http://dx.doi.org/10.33448/rsd-v12i5.41725
CrossRef - Martins S. C. R., Marques M. C., Vidal M. G., Moreira P. H., Tolentino P., Dinelli R. G., Fernandes G. V. O., Shibli J. A. Is the facial bone wall critical to achieving esthetic outcomes in immediate implant placement with immediate restoration? A systematic review. Adv Clin Exp Med. 2024;33(9):979-997. doi:10.17219/acem/173573
CrossRef - Campi M., Leitão-Almeida B., Pereira M., Shibli J. A., Levin L., Fernandes J. C. H., Fernandes G. V. O., Borges T. F. Immediate implant placement in damaged extraction sockets: A systematic review and meta-analysis of randomized controlled trials. Quintessence Int. 2025;56(1):34-45. doi: 10.3290/j.qi.b5768294
- Otero A. I. P., Fernandes J. C. H., Borges T., Nassani L., Castilho R. M., Fernandes G. V. O. Sinus lift associated with Leucocyte-Platelet Rich Fibrin (second generation) for bone gain: a systematic review. J Clin Med. 2022;11(7):1888. doi: 10.3390/jcm11071888
CrossRef - Fontenelle A. T. S. P. All-on-Four: revisão de literatura [monografia]. São Luís/MA, Brazil: Faculdade Sete Lagoas – FACSETE; 2024 [acesso em 14 maio 2025]. Available at: https://rdta.facsete.edu.br/monografia/files/original/75377e111380933cdf8dd23119e07f1b.pdf
- Pellizzer K., Paz J. D. Implantes dentários: técnica All-on-Four. J Multidiscipl Dent. 2023;13(2):51-55. doi.org/10.46875/jmd.v13i2.915
CrossRef - Dioguardi M., Spirito F., Quarta C., Sovereto D., Basile E., Ballini A., Caloro G. A., Troiano G., Muzio L. L., Mastrangelo F. Guided Dental Implant Surgery: Systematic Review. J Clin Med. 2023;12(4):1490. doi: 10.3390/jcm12041490
CrossRef - Baskaran P., Prakash P. S. G., Appukuttan D., Mugri M. H., Sayed M., Subramanian S., Al Wadei M. H. D., Ahmed Z. H., Dewan H., Porwal A., Balaji T. M., Varadarajan S., Heboyan A., Fernandes G. V. O., Patil S. Clinical and radiological outcomes for guided-implant placement in sites preserved with bioactive glass bone graft after tooth extraction: A controlled clinical trial. Biomimetics. 2022;7:43.
CrossRef - Aghaloo T., Hadaya D., Schoenbaum T. R., Pratt L., Favagehi M. Guided and Navigation Implant Surgery: A Systematic Review. Int J Oral Maxillofac Implants. 2023;38(suppl):7-15. doi: 10.11607/jomi.10465
CrossRef - Costa B. E., Bueno C. R., Momesso N. R., Duarte G. L. C., Junior P. D. R., Lopes M. H. Management for the rehabilitation of atrophic mandible fracture: case using a conservative approach and short implants. Res Soc Developm. 2022;11(4):e4611424249.
CrossRef - Carvalho L. F., Carvalho L. P., Sotto-Maior B. S., Dias A. L., Bezerra F. J. B., Bergamo E. T. P., Carvalho A. M. Rehabilitation of Atrophic Maxilla with Immediate Loading of Extrasinus Zygomatic Implant. J Craniofac Surg. 2022;33(5):e488-e491. doi: 10.1097/SCS.0000000000008411
CrossRef - Ali S. A., Karthigeyan S., Deivanai M., Kumar A. Implant Rehabilitation for Atrophic Maxilla: A Review. J Indian Prosthodont Soc. 2014;14(3):196-207. doi: 10.1007/s13191-014-0360-4
CrossRef - Vaira L. A., Biglio A., Roy M., Salzano G., Troise S., Abbate V., Mayo-Yanez M., Lechien J. R., Piombino P., De Riu G. Full-arch rehabilitation of severely atrophic maxilla with additively manufactured custom-made subperiosteal implants: A multicenter retrospective study. J Craniomaxillofac Surg. 2024;52(9):991-998. doi: 10.1016/j.jcms.2024.06.016
CrossRef - Fernandes G. V. O., Ferreira N. R. N., Heboyan A., Nassani L. M., Pereira R. M. A., Fernandes J. C. H. Clinical assessment of short implants (>6mm and ?8.5mm) in posterior sites with an average follow-up of 74 months: A retrospective study with the re-assessment of patients. Int J Oral Maxillofac Implants. 2023;38(5):915-926.
CrossRef - Badaró M. M., Marin D. O. M., Pauletto P., Gonçalves T. M.. S. V., Porporatti A. L., Canto G. D. L. Failures in Single Extra-Short Implants (? 6 mm): A Systematic Review and Meta-analysis. Int J Oral Maxillofac Implants. 2021;36(4):669-689. doi: 10.11607/jomi.8689
CrossRef - Gürlek Ö., Kaval M. E., Buduneli N., Nizam N. Extra-short implants in the prosthetic rehabilitation of the posterior maxilla. Aust Dent J. 2019;64(4):353-358. doi: 10.1111/adj.12711
CrossRef - Deste G., Durkan R. Effects of all-on-four implant designs in mandible on implants and the surrounding bone: A 3-D finite element analysis. Niger J Clin Pract. 2020;23(4):456-463. doi: 10.4103/njcp.njcp_471_19
CrossRef - Tezeri?ener H. A., Özalp Ö., Altay M. A., Sindel A. Comparison of stress distribution around all-on-four implants of different angulations and zygoma implants: a 7-model finite element analysis. BMC Oral Health. 2024;24(1):176. doi: 10.1186/s12903-023-03761-x
CrossRef - Galindo D. F., Butura C. C. Immediately loaded mandibular fixed implant prostheses using the all-on-four protocol: a report of 183 consecutively treated patients with 1 year of function in definitive prostheses. Int J Oral Maxillofac Implants. 2012;27(3):628-633.
- Amaral B. S., Costa M. T. A., Almeida V. S., Silva R. C., Barros M. L. T., Junior J. S. Reabilitação da Maxila Atrófica com a Técnica All-on-Four Híbrida Associada a Implantes Pterigóides: Relato de Caso. Braz J Case Rep. 2025;5(1):bjcr66. doi: 10.52600/2763-583X.bjcr.2025.5.1.bjcr66.
CrossRef





