.jpg)
Functional Oral Self-Mutilation in Children: A Clinical Case Series
Marília Goulardins Gomes*  , Ana Paula Dias Moreno , Letícia Santana Fernandes , Fernanda Souza Liévana and Andiara De Rossi
, Ana Paula Dias Moreno , Letícia Santana Fernandes , Fernanda Souza Liévana and Andiara De Rossi
1Department of Pediatric Dentistry, School of Dentistry of Ribeirão Preto, University of São Paulo, Ribeirão Preto, Brazil .
http://dx.doi.org/10.12944/EDJ.07.0102.09
Functional oral self-mutilation is an uncommon behavioral condition in children without neurological or syndromic disorders. It may cause significant soft-tissue injury and requires careful diagnosis and interdisciplinary management.
This report describes three pediatric cases with distinct patterns of functional oral self-mutilation. The first case involved a 6-year-old boy who presented with periungual trauma resulting from repetitive nail-biting. The second case described a 7-year-old boy who developed a localized gingival lesion adjacent to tooth 54 due to habitual scratching with the fingernail. The third case involved a 9-year-old girl who exhibited recurrent trauma to the labial and buccal mucosa caused by digital manipulation. All patients received individualized care including oral hygiene instruction, behavioral guidance, and psychological referral.
Functional oral self-mutilation represents a behavioral challenge that requires early recognition and multidisciplinary intervention. Caregiver education, psychological support, and preventive dental management are essential for long-term control and prognosis.
Copy the following to cite this article:
Gomes M. G, Moreno P. D, Fernandes L. S, Liévana F. S, Rossi A. D, Functional Oral Self-Mutilation in Children: A Clinical Case Series. Enviro Dental Journal 2025; 7(1-2).
DOI:http://dx.doi.org/10.12944/EDJ.07.0102.09Copy the following to cite this URL:
Gomes M. G, Moreno P. D, Fernandes L. S, Liévana F. S, Rossi A. D, Functional Oral Self-Mutilation in Children: A Clinical Case Series. Enviro Dental Journal 2025; 7(1-2). Available here:https://bit.ly/4q7xpIK
Download article (pdf) Citation Manager

Introduction
Self-mutilation is defined as intentional, self-inflicted tissue damage without conscious intent to cause death1,2. It represents a significant public health concern, with rising prevalence among adolescents and young adults and affecting individuals across different demographic and socioeconomic groups³. Reported prevalence rates reach 4% in adults, 17–38% among university students, and up to 69% among youth exposed to social vulnerability4.
In Brazil, Law No. 13.819/2019 established a national framework for the prevention of self-mutilation and suicide, reinforcing strategies for mental health promotion and mandating surveillance, reporting, and educational measures across health and social sectors5.
The diagnosis of oral self-mutilation is complex because lesions may present in varied clinical patterns and resemble multiple other conditions6. A comprehensive evaluation is needed to distinguish these injuries from habitual behaviors, aesthetic manipulations, or manifestations of psychiatric disorders¹. Recent reviews indicate that oral self-injurious behavior in children and adolescents may be influenced by neurological, genetic, psychiatric, and psychosocial factors, including adverse experiences and social vulnerability.7,8
Oral self-mutilation is broadly categorized into organic and functional forms. The organic type occurs in individuals with genetic syndromes or neurological impairments such as Lesch–Nyhan syndrome, sensory neuropathies, or autism spectrum disorders, characteristically presenting as early-onset, involuntary, and repetitive behavior.9,10
The functional type, however, affects individuals without detectable systemic conditions, in whom trauma is intentionally inflicted in response to emotional distress, frustration, or interpersonal conflict. These behaviors are typically repetitive and socially inappropriate, and may result in mild to moderate soft-tissue injury. Emotional triggers such as family instability, school-related stress, parental separation, or sibling loss are frequently observed¹. Functional cases are further divided into injuries superimposed on pre-existing lesions, habits that lead to destructive behavior, and injuries of unclear or multifactorial psychological origin¹.Patients with functional oral self-mutilation often display common behavioral characteristics: the actions are socially inappropriate, repetitive, and result in mild to moderate soft tissue damage6.
Some individuals develop functional oral self-mutilation specifically involving gingival tissues, the most commonly affected site. This is especially observed in pediatric female patients who use objects such as pencils or their own fingernails to induce trauma¹.Evidence suggests that nearly 70% of pediatric cases can be fully resolved through timely and interdisciplinary management.11Effective care should combine psychological evaluation, behavioral support, pharmacological therapy when indicated, and the use of protective intraoral devices, with surgical approaches reserved for selected cases. 2,10
The present study describes three pediatric presentations of behaviorally induced functional oral injury, all occurring in the absence of identifiable genetic disorders, and highlights the relevance of differential diagnosis and multidisciplinary strategies in dental practice.
Case Report
Case 1:
A 6-year-4-month-old male patient attended the undergraduate pediatric dentistry clinic of a public university for dental treatment. During anamnesis, the caregiver reported that the child was undergoing neurological follow-up and pharmacological management for anxiety and hyperactivity. The patient was generally communicative with other children but occasionally displayed aggressive behavior and had learning difficulties at school. The caregiver also noted onychophagia, object biting, and self-inflicted trauma characterized by habitual removal of periungual cuticles.
Clinical examination confirmed ongoing self-injurious behavior, with multiple lesions surrounding the fingernails caused by repetitive biting and cuticle removal (Figure 1A, Figures 1B–1E). Based on history and clinical presentation, the diagnosis was functional self-mutilation involving the periungual tissues. Management included behavioral guidance, counseling on habit interruption, reinforcement of oral and hand hygiene, and referral for psychological support due to the emotional and behavioral context associated with the habit.
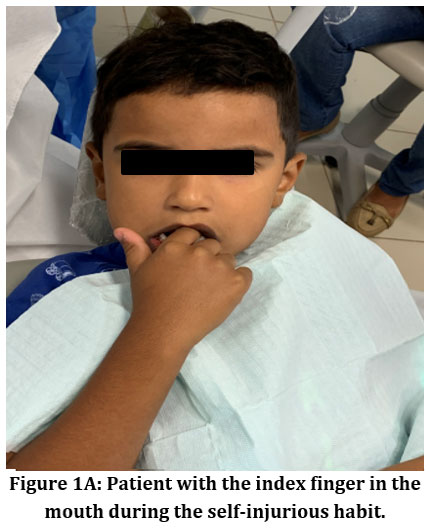 | Figure 1A: Patient with the index finger in the mouth during the self-injurious habit.
|
 | Figure 1B: Patient showing finger injury caused by the habit of biting and removing the cuticles.
|
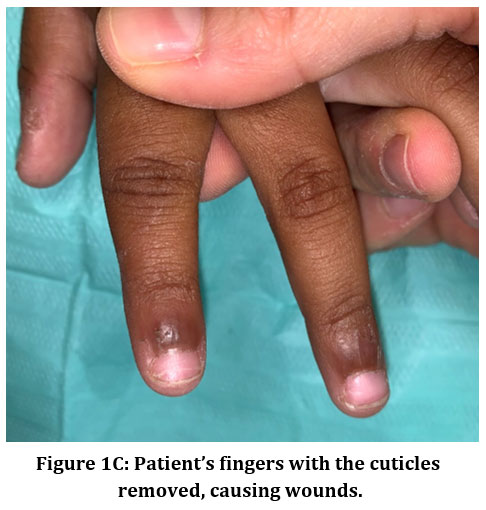 | Figure 1C: Patient’s fingers with the cuticles removed, causing wounds.
|
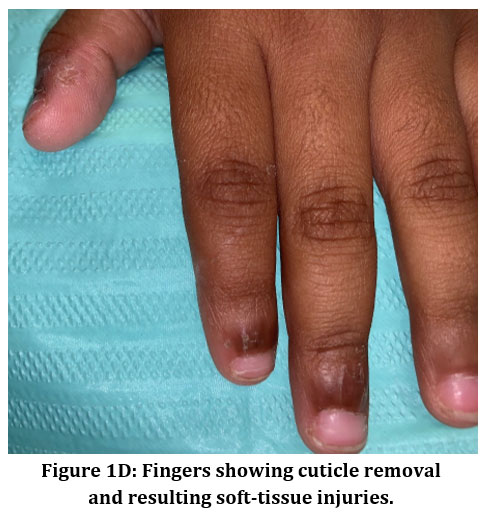 | Figure 1D: Fingers showing cuticle removal and resulting soft-tissue injuries.
|
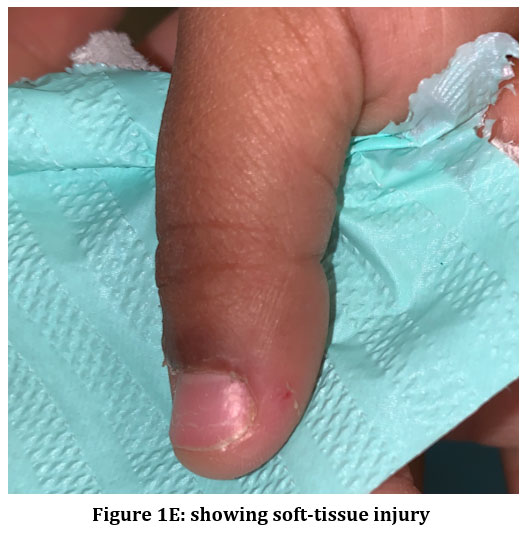 | Figure 1E: showing soft-tissue injury
|
Case 2
A 7-year-2-month-old male patient attended the undergraduate pediatric dentistry clinic of a public university for dental treatment. In the intraoral clinical examination, a unilateral lesion was observed on the free gingiva adjacent to the buccal surface of tooth 54 (Figures 2D and 2E), caused by a self-injurious behavior characterized by “picking” the gingival tissue with the right index fingernail (Figures 2A–2C). No similar lesions were present in other oral regions.
The self-mutilating habit resulted in gingival recession, edema, and bleeding affecting the buccal and free gingival margins in the area of tooth 54 (Figure 2D). The clinical diagnosis was functional self-mutilation, since the child was physically healthy and presented no neurological or syndromic conditions. The patient received detailed oral-hygiene instruction to prevent infection and support healing, along with referral for psychological care.
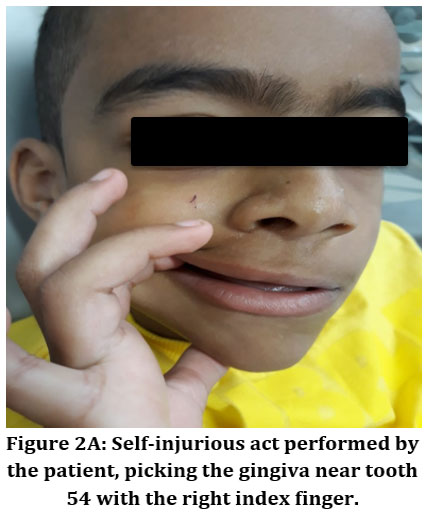 | Figure 2A: Self-injurious act performed by the patient, picking the gingiva near tooth 54 with the right index finger.
|
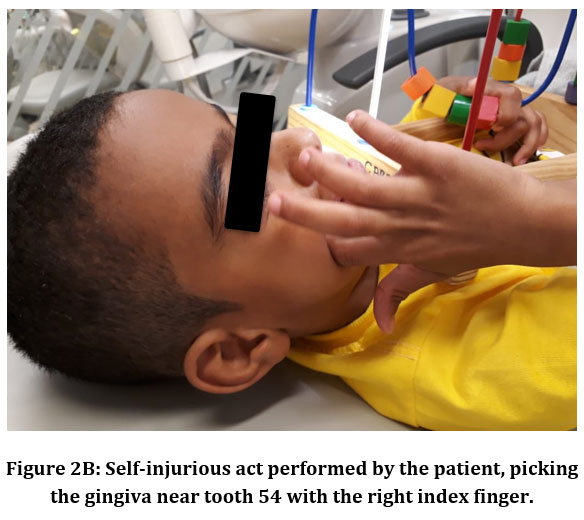 | Figure 2B: Self-injurious act performed by the patient, picking the gingiva near tooth 54 with the right index finger.
|
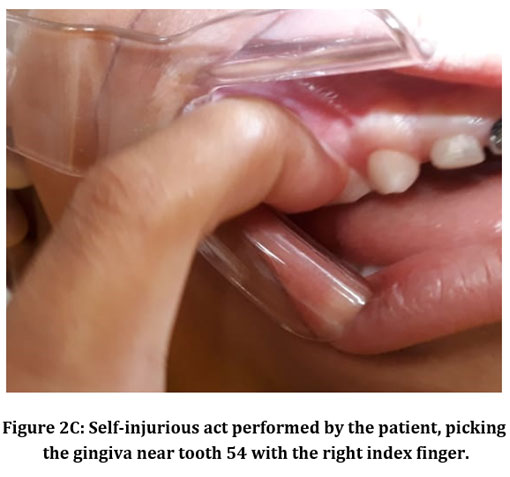 | Figure 2C: Self-injurious act performed by the patient, picking the gingiva near tooth 54 with the right index finger.
|
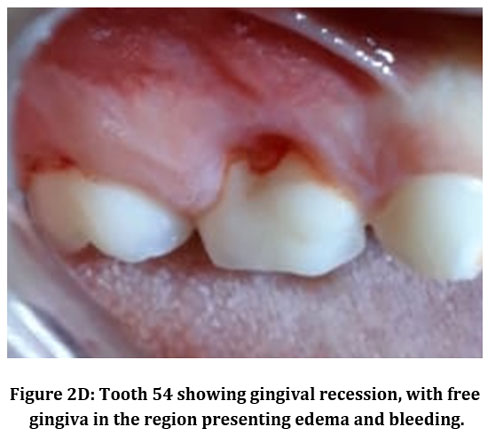 | Figure 2D: Tooth 54 showing gingival recession, with free gingiva in the region presenting edema and bleeding.
|
CASE 3
A 9-year-old female patient attended the undergraduate pediatric dentistry clinic of a public university for dental treatment. Clinical examination revealed a self-injurious habit in which the patient used her fingers to stretch the lower labial mucosa and both buccal mucosae (Figures 3A–3C), causing soft-tissue injury and bleeding. Her medical history and anamnesis showed no behavioral disorders or features suggestive of syndromic conditions. Therefore, the diagnosis was functional self-mutilation. The management plan included psychological referral to identify emotional triggers and support behavioral regulation, in addition to preventive oral-care guidance.
.jpg) | Figure 3A: Injuries on the right buccal mucosa
|
 | Figure 3B: Injuries on the left buccal mucosa
|
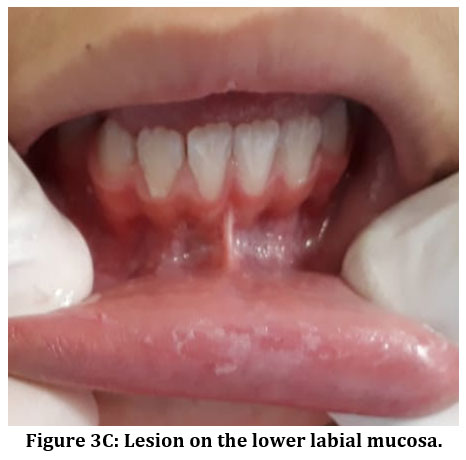 | Figure 3C: Lesion on the lower labial mucosa.
|
Discussion
Functional oral self-mutilation in children is a multifactorial condition influenced by the interaction of emotional, cognitive, biological, environmental, and behavioral components6,13,14. The three cases described in this report illustrate distinct clinical manifestations of self-injurious behavior in the absence of neurological or syndromic disorders, highlighting the heterogeneous nature of functional self-mutilation in pediatric patients.
In Case 1, the periungual trauma reflected a repetitive and socially inappropriate pattern characteristic of functional self-injury6,13. Environmental context played a notable role, as limited maternal involvement constituted a significant stressor and may have contributed to the child’s reliance on self-inflicted behaviors as a means of emotional regulation6,14,15. Biological factors were also relevant, as anxiety and hyperactivity are associated with neurobiological alterations in emotional-regulation pathways6,12,15. Cognitive interpretations of stress—particularly those involving attachment and perceived security—may have contributed to the persistence of the behavior¹³. Affective dysregulation, marked by anxiety, tension, and distress, likely acted as a recurrent trigger6,14. Behavioral difficulties, including interpersonal conflict and academic challenges, further reinforced the habitual pattern of self-injury6,15. Importantly, the cumulative evidence in the literature indicates that when functional self-mutilation is not identified and addressed early, the behavior may persist, intensify, or become chronic into adulthood.
Case 2 demonstrated how functional self-mutilation may affect gingival tissues, particularly in areas easily accessible to the child1,16. Gingival picking with the fingernail resulted in localized inflammation, recession, and bleeding—findings consistent with previous descriptions of self-inflicted gingival trauma4,16. As these lesions often become evident only when advanced or visibly destructive, early detection relies heavily on caregiver vigilance2,4.While local measures such as hygiene instruction support soft-tissue healing, psychological referral is crucial to address the emotional and behavioral triggers underlying the injury2,4,18.
Case 3 illustrated another form of functional self-mutilation involving manipulation of the labial and buccal mucosa. The absence of behavioral or syndromic findings confirmed the functional etiology. This presentation aligns with the broad spectrum of self-injurious behaviors—including mucosal manipulation, biting, scratching, and rubbing—each influenced by emotional state and preferred mechanism of injury4,18. As with the previous cases, psychological assessment is a central component of management, enabling identification of emotional triggers and implementation of individualized behavioral-regulation strategies. Cognitive-behavioral approaches are particularly valuable in functional cases, as they facilitate the development of healthier coping mechanisms4,2,12.
The therapeutic modalities described in the literature reflect the wide spectrum of self-injurious behaviors. Psychological interventions,such as positive reinforcement, overcorrection, and sensory alternatives,remain first-line treatments because they provide favorable outcomes with minimal adverse effects??¹?. In contrast, organic self-mutilation, particularly that observed in Lesch–Nyhan syndrome, involves distinct and more complex etiological mechanisms. This X-linked metabolic disorder is characterized by a deficiency of the enzyme hypoxanthine-guanine phosphoribosyltransferase (HPRT), leading to uric acid overproduction and dopaminergic dysfunction in the basal ganglia. As a result, patients exhibit severe and specific patterns of self-injury, especially biting of the lips, tongue, and fingers, due to a neurobiological inability to inhibit self-aggressive behaviors????¹?. Consequently, management usually requires a combination of behavioral, restrictive, and pharmacological strategies.
Pharmacological approaches—including tricyclic antidepressants, dopamine-receptor antagonists, anticonvulsants, and serotonergic agents—show variable effectiveness and are generally recommended for organic etiologies??¹?. Although botulinum toxin type A may reduce bite force, its use has not consistently decreased the frequency of self-injurious episodes??¹??¹?.
Beyond genetic and metabolic conditions, another important etiological domain involves Body-Focused Repetitive Behaviors (BFRBs), such as onychophagia, lip biting, and cheek-mucosa biting. BFRBs are frequently associated with anxiety, impulsivity, and neurodevelopmental disorders, representing key differential diagnoses when assessing oral self-injurious behavior. Considering these mechanisms broadens the etiological understanding of oral self-injury and reinforces the need for a multidisciplinary, individualized clinical approach.6,10,20,21
Protective strategies such as physical restraint or intraoral devices may be necessary in severe or refractory cases. Intraoral appliances can prevent new injuries by separating the traumatized tissues from the teeth and may assist healing, but their use requires clinical expertise and may involve frequent adjustments4,11,17. When all conservative measures fail, tooth extraction may be considered; although radical, it can significantly reduce tissue damage and prevent deformities associated with repeated trauma4,10,16.
Taken together, the three cases in this report illustrate the wide clinical spectrum of functional oral self-mutilation and emphasize that successful management requires an individualized, multidisciplinary approach. Early recognition is fundamental to preventing lesion progression, recurrence, and long-term persistence, thereby promoting healthier emotional regulation during childhood and reducing the likelihood that the behavior will continue into adult life.
Conclusion
Functional oral self-mutilation in children presents significant diagnostic and therapeutic challenges due to its behavioral and emotional origins. Health professionals must remain vigilant for potential signs of self-inflicted oral injury, as clinical manifestations are varied and may resemble other pathological conditions. Therefore, a thorough differential diagnosis is essential to exclude comorbidities and establish an appropriate treatment plan.Successful management requires not only prompt identification, psychological support, and preventive dental care but also close interdisciplinary collaboration among dental practitioners, mental health professionals, and caregivers. The active participation of parents and family members is fundamental for patient monitoring and relapse prevention.Therapeutic strategies should be individualized, considering the underlying cause of the behavior, the affected structures, the severity of the lesions, and the presence or absence of associated comorbidities, to ensure a comprehensive and effective approach to rehabilitation and the maintenance of stable clinical results.
Acknowledgement
The authors would like to express their gratitude to the pediatric dentistry clinical staff and academic colleagues from the School of Dentistry of Ribeirão Preto, University of São Paulo, for their valuable support during patient care and case documentation. The authors also thank the participating children and their families for their collaboration and trust.
Funding Statement
The author(s) received no financial support for the research, authorship, and/or publication of this article
Conflict of Interest
The authors declare that there are no conflicts of interest related to the publication of this case report.
Data Availability Statement
The manuscript incorporates all information and clinical observations obtained during the reported cases. No additional datasets were generated or analyzed during the current study.
Ethical Statement
The study was conducted in accordance with the ethical standards of the institutional and national research committees and with the 1964 Helsinki Declaration and its later amendments. Ethical approval was granted by the Research Ethics Committee of the Faculty of Dentistry of Ribeirao Preto, University of São Paulo (CAAE: 39685920.7.0000.5419). Written informed consent was obtained from the parents or legal guardians of all participants for their participation and for the publication of clinical photographs. The identities of the participants were fully protected, and all images were used solely for scientific and educational purposes.
Informed Consent Statement
Written informed consent was obtained from the parents or legal guardians of all participating children, in accordance with the ethical standards and regulations of the country of origin. All procedures adhered to the principles outlined in the Declaration of Helsinki. The privacy and confidentiality of all participants were strictly protected.
Clinical Trial Registration
This research does not involve any clinical trials
Author Contributions
Marília Goulardins Gomes: Conceptualization, Methodology, Data Collection, Writing – Original Draft, Writing – Review & Editing.
Ana Paula Dias Moreno: Supervision, Methodology, Writing – Review & Editing.
Letícia Santana Fernandes: Data Collection, Visualization, Writing – Review & Editing.
Fernanda Souza Liévana: Methodology, Validation, Writing – Review & Editing.
Andiara De Rossi: Supervision, Project Administration, Writing – Review & Editing.
References
- Hildebrand C, Borkovic M, Melsen B. Self-inflicted gingival injuries in children: diagnosis and management. J Clin Pediatr Dent. 2011;35(4):335–340.
- Limeres J, Feijoo JF, Baluja F, Seoane J, Diz P. Self-inflicted gingival injury by a child: a case report. Int J Paediatr Dent. 2013;23(5):374–378.
- Bezerra K, Nascimento F, et al. Self-mutilation among adolescents: a systematic review with meta-analysis. Texto Contexto Enferm. 2023;32:e20230032.
CrossRef - Limeres J, Feijoo JF, Baluja F, Seoane J, Diz P, Diniz M, et al. Oral self-injury: an update. J Clin Periodontol. 2013;40(Suppl 15):77–86.
- Brazil. Law No. 13,819 of April 26, 2019. Diário Oficial da União. 2019.
- Cannavale C, Marini A, Lucarelli L, Daneluzzo E. Self-harm behavior: an integrative model and implications for clinical practice. J Child Adolesc Behav. 2015;3(5):1–7.
- Melo JRT, Oliveira NMC, Rosendo CP, Barreira AK, Colares V. Oral self-mutilation in children and adolescents: integrative review. Res Soc Dev. 2021;10(2):e12493.
CrossRef - Melo JRT, Rangel AL, Freitas JM, Cardozo D, Silva FP, Costa AMA, et al. Assessment of self-injurious behavior and oral lesions among adolescents in foster care. J Public Ment Health. 2023;22(3):190–201.
- Campollo J, Barajas E, Martínez P, Esquivel F, Robledo M. Self-injurious behavior in Lesch–Nyhan syndrome: oral manifestations and management. J Clin Exp Dent. 2018;10(6):e577–e581.
- Galeotti A, Pardo M, Bertini M, Pieragostini A, Festa P, Gatto R. Oral self-inflicted trauma in infants with cerebellar hypoplasia: dental management case report. J Clin Pediatr Dent. 2024;48(2):95–99.
- Cantile T, Valletta A, Salza E, Paglia L, Ferrazzano GF. Self-inflicted oral-dental mutilations (SIODMs) in paediatric patients: a systematic review. Eur J Paediatr Dent. 2025;26(1):12–22.
- Franklin JC, Puzia ME, Lee KM, Hanna EK, Spring VL, Lopez FA, et al. Nonsuicidal self-injury: key research themes and future directions. Annu Rev Clin Psychol. 2018; 14:339–363.
- Zetterqvist M. The DSM-5 diagnosis of nonsuicidal self-injury disorder: a review of the empirical literature. Child Adolesc Psychiatry Ment Health. 2015; 9:31.
CrossRef - Plener PL, Kapusta ND, Brunner R, Kaess M. Non-suicidal self-injury in children and adolescents: prevalence, risk factors and treatment. Curr Opin Psychiatry. 2021;34(6):605–611.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5-TR. 5th ed. American Psychiatric Association; 2022.
CrossRef - Cho SY, Kim HJ, Park JH. Oral self-injurious behavior in a child with normal development: clinical features and management. Pediatr Dent. 2020;42(3):240–243.
- Vento-Zahra E, Grech J, Mallia J, Camilleri S. Self-inflicted oral lesions in children: a review and case report. BMC Oral Health. 2019; 19:284.
- Garrocho-Rangel A, Herrera-Bernal G, Soto-González M, Pozos-Guillén A. Oral self-injury in children and adolescents: a systematic review. Spec Care Dentist. 2018;38(5):345–352.
- Favazza AR. Bodies Under Siege: Self-Mutilation, Nonsuicidal Self-Injury, and Body Modification in Culture and Psychiatry. 3rd ed. Johns Hopkins University Press; 2011.
- Najera DB. Body-focused repetitive behaviors: Beyond bad habits. JAAPA. 2022 Feb 1;35(2):28-33. doi: 10.1097/01.JAA.0000817812.38558.1a. PMID: 34985009.
CrossRef - Roberts S, O'Connor K, Aardema F, Bélanger C. The impact of emotions on body-Focused repetitive behaviors: evidence from a non-treatment-seeking sample. J Behav Ther Exp Psychiatry. 2015 Mar; 46:189-97. doi: 10.1016/j.jbtep.2014.10.007. PMID: 25460266.
CrossRef





