.jpg)
Salivary screening for Selenomonas noxia in the oral cavity of pediatric patients
Rachelle Davidowitz1 , Katherine M. Howard2* and Karl Kingsley2 
1Department of Pediatrics, University of Nevada, School of Dental Medicine, Las Vegas, Nevada US .
2Department of Biomedical Sciences, University of Nevada, School of Dental Medicine, Las Vegas, Nevada US .
http://dx.doi.org/10.12944/EDJ.01.01.01
The oral microbiome may be affected by patient medications, disease conditions and systemic disorders. Selenomonas noxia is an anaerobic, motile, non spore-forming, gram-negative rod that has been repeatedly associated with periodontal disease and other disorders, including obesity. Based upon the paucity of evidence regarding oral prevalence, the objective of was to evaluate S. noxia prevalence by sampling saliva from the oral cavity to screen for this pathogen. Using an existing saliva repository, DNA was isolated and screened using quantitative real-time polymerase chain reaction (qPCR). Demographic analysis of study samples and qPCR results was also performed. Approximately half of the samples (n=96) were derived from females (51%) and the majority were from Hispanic patients (62.5%). Following DNA isolation and qPCR screening 37.5% (n=35) were found to harbor S. noxia DNA, which was more prevalent among the samples derived from adults (n=22 or 22.9%) than pediatric patients (n=13 or 13.5%). This study provides novel information regarding the oral prevalence of S. noxia among both pediatric and adult populations from a dental school population. These data are an important part of the overall epidemiologic analysis of this organism and may provide some initial information regarding the risk for periodontal or other health issues related to the presence among these populations.
Copy the following to cite this article:
Davidowitz R, Howard K. M, Kingsley K. Salivary screening for Selenomonas noxia in the oral cavity of pediatric patients. Enviro Dental Journal 2019; 1(1).
DOI:http://dx.doi.org/10.12944/EDJ.01.01.01Copy the following to cite this URL:
Davidowitz R, Howard K. M, Kingsley K. Salivary screening for Selenomonas noxia in the oral cavity of pediatric patients. Enviro Dental Journal 2019; 1(1). Available from: https://bit.ly/31Xz5dv
Download article (pdf) Citation Manager
Introduction
The oral microbiome may be affected by patient medications, disease conditions and systemic disorders.1,2 For example, specific microflora may be associated with diseases of the oral cavity like caries, periodontal disease and oral cancer.3-5 In fact, many studies have demonstrated strong correlations between the oral microbiome and periodontal disease across the lifespan.6,7
Selenomonas noxia is an anaerobic, motile, non spore-forming, gram-negative rod that has been repeatedly associated with periodontal disease.8,9 More specifically, it has been found in cases of generalized aggressive periodontitis and chronic periodontitis, as well as gastric ulcers.10, 11 Besides the relation between S. noxia and periodontal disease, some studies have found an association between S. noxia and obesity.12,13 These correlations have been a driving force towards the development of screening tools to detect and identify this oral pathogen.8,13,14
These data suggest that the composition of salivary bacteria changes could function as a biological indicator of developing periodontal disease and/or obesity, although few studies have examined oral prevalence of this organism.15,16 Based upon the paucity of evidence regarding oral prevalence, the objective of was to evaluate S. noxia prevalence by sampling saliva from the oral cavity to screen for this pathogen.
Methodology
Human Subjects
This project was reviewed and approved by the Institutional Review Board (IRB) and Office for the Protection of Human Research Subjects (OPRS) at the University of Nevada, Las Vegas (UNLV) under Protocol# 1502-5068M. The original approved collection protocol OPRS#880427-1 was titled “The Prevalence of Oral Microbes in Saliva from the University of Nevada Las Vegas (UNLV) School of Dental Medicine (SDM) pediatric and adult clinical population”.
Sample Collection
This was a retrospective study of previously collected saliva samples, stored in an existing biomedical repository. In brief, all samples were taken from UNLV-SDM clinic patients that previously provided Informed Consent (Adults) or Pediatric Assent (Children). At the time of sample collection, each sample was assigned a non-duplicated, randomly generated number to prevent any linkage with the patient information or other patient-specific information. Basic demographic information was collected for each sample (Sex, Age, Race/Ethnicity) with no other information that could be linked to the original voluntary study participants.
Each study participant was provided with a sterile 50 mL container for unstimulated saliva collection and asked to provide up to 5.0 mL in total. Each sample was transferred on ice to the biomedical laboratory and kept at -80C.
The original sampling protocol required patients to provide Informed Consent (adult) and Pediatric Assent (pediatric) prior to the collection of saliva. The inclusion criteria were pediatric patients aged seven (7) years or older and their parents or guardians who agreed to participate. Pediatric assent and Parental permission to consent for voluntary participation were obtained at the time of study enrollment. Adult parents or guardians provided Informed Consent. Exclusion criteria included any person that was not a patient of record at UNLV-SDM, any patients who declined to participate, and any parent or guardian that declined to let their child participate.
DNA Isolation
Each sample was then thawed and 1.0 mL was used for DNA isolation. The GenomicPrep DNA isolation kit from Amersham Biosciences (Buckinghamshire, UK) was used, according to the procedure recommended by the manufacturer. DNA isolations were subsequently screening using a NanoDrop spectrophotometer from ThermoFisher (Fair Lawn, NJ). Absorbance readings at A230, A260 and A80 were collected and analyzed for DNA concentration, purity and contamination. The A260:A280 ratio was used to calculate the initial purity and the A260:A230 ratio was used as a secondary measure of nucleic acid purity and potential contamination.
PCR Screening
All samples with sufficient DNA quantity (> 1.0 ng/uL) and sufficient DNA purity (A260:A280 ratio greater than 1.65) were then processed using quantitative real-time polymerase chain reaction (qPCR). In brief, qPCR used initial incubation of 50C for 120 seconds, followed by denaturation at 95C for ten minutes and 40 cycles, consisting of 95C for 15 seconds and 60CC for 60 seconds. Positive control human glyceraldehyde 3-phosphate dehydrogenase (GAPDH) and standards were derived from American Type Culture Collection (ATCC) S. noxia reference strains ATCC-43541, -51893, and -700225), as previously described [13,15,16].
Positive Control
Glyceraldehyde- 3- phosphate dehydrogenase (GAPDH)
GAPDH 5’-ATCTTCCAGGAGCGAGATCC-3’ (sense); 20 nt; 55% GC; Tm=66C
GAPDH 5’-ACCACTGACACGTTGGCAGT-3’ (antisense); 20 nt; 55%GC; Tm=70C
Optimal PCR Tm: 65C
Forward primer- SNF1, TCTGGGCTACACACGTACTACAATG (25 bp)
Reverse primer- SNR1, GCCTGCAATCCGAACTGAGA (20 bp)
SnP[ 6 ~ FAM]CAGAGGGCAGCGAGAGAGTGATCTTAAGC [TAMRA]
The selected probe (SnP) was labeled with the reporter dye 6-carboxyfluorescein (FAM) at the 5’-end and with the reporter dye tetramethyl-6-carboxyrhodamine (TAMRA) at the 3’-end.
Statistical Analysis
Basic demographic information was compiled and presented using descriptive statistics. Analysis of these demographics was performed using non-parametric statistics (Chi square). Results of the qPCR screening were also analyzed using descriptive statistics and Chi square analysis.15,16
Results
The demographic information for all potential saliva samples was organized and analyzed (Table1). These data demonstrated that slightly more than half of samples (56.3%, n=54/96) were derived from pediatric patients, with the remainder from adult patients (43.7%, n=42/96), which was similar to the demographics of the overall clinic population. The majority of these patients were Hispanic (minority) 76.1%, which was higher than the overall percentage from the UNLV-SDM clinic population (58.6%). The average age and range of the pediatric samples (5-17 yrs, 12.9 yrs) was slightly higher than the average of the pediatric clinic in general – mainly due to the ability of subjects to provide Pediatric Assent and provide sufficient sample quantity. The average age and range of the adult samples (18-73 yrs, 43.1 yrs>) was slighty lower than the overall clinic population – presumably due to random variations in the clinic patients present on the specific days of the initial study sample collection.
Table 1: Demographic analysis of patient samples.
| Study sample (n=96) | UNLV-SDM clinic | Statistical analysis | |
| Sex | |||
| Female | 51.0% (n=49) | 50.90% | c2=0.004, d.f.=1 |
| Male | 49.0% (n=47) | 49.10% | p=0.9496 |
| Race / Ethnicity | |||
| White | 23.9% (n=23) | 41.40% | c2=126.235, d.f.=1 |
| Minority | 76.1% (n=73) | 58.60% | p=0.0001 |
| Hispanic | 62.5% (n=60) | 35.90% | |
| Black | 7.3% (n=7) | 13.10% | |
| Asian / Other | 6.3% (n=6) | 9.60% | |
| Age | |||
| Pediatric | Range: 5 – 17 yrs. | Range: 0 – 17 yrs. | |
| (n=54) | Ave.=12.9 yrs. | Ave.=10.14 yrs. | |
| Adult | Range: 18 – 73 yrs. | Range: 18 – 91 yrs. | |
| (n=42) | Ave.=43.1 yrs. | Ave.=52.3 yrs. |
Each of the saliva samples were processed to extract DNA for PCR screening and analysis (Table 2). These data demonstrated a yield (recovery rate) of 100%, which was slightly more than the expected range according to the manufacturer protocol (90-95%). The concentration of DNA isolated from the saliva samples was 521.26 ng/uL, which was well within the expected range according to the manufacturer protocol (100 – 1000 ng/uL). The DNA quality or purity as measured by the ratio of absorbance readings at 260 and 280 nm demonstrated an average of 1.645, which is close to the average range according to the manufacturer protocol (1.7 – 2.0).
Table 2: DNA isolation and study sample analysis.
| DNA concentration | DNA purity | Recovery/yield | |
| Study sample | 521.26 ng/uL +/- 92.9 | A260:A280=1.645 | 100% (n=96) |
| Manufacturer range | 100 – 1000 ng/uL | 1.70-2.00 | 90-95% |
The DNA isolated from each patient sample was then screened for the presence of the positive control - human glycolytic pathway enzyme glyceraldehyde 3-phosphate dehydrogenase (GAPDH) (Figure 1). These data revealed that all samples screened using PCR were found to harbor GAPDH above the limit of detection (LOD). Each sample was then sorted by age and graphed, which did not reveal any patterns based upon the age of the patient and the signal band intensity (SBI).
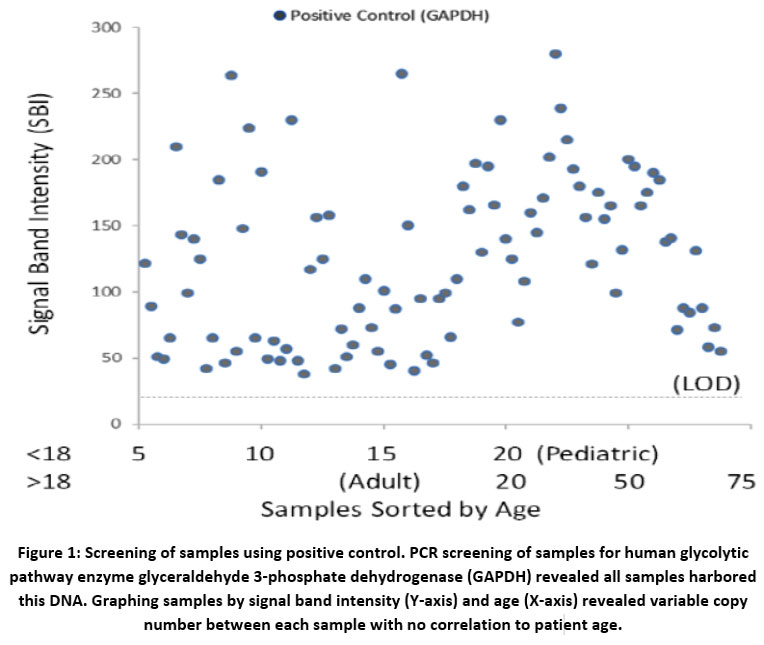 | Figure 1: Screening of samples using positive control. PCR screening of samples for human glycolytic pathway enzyme glyceraldehyde 3-phosphate dehydrogenase (GAPDH) revealed all samples harbored this DNA. Graphing samples by signal band intensity (Y-axis) and age (X-axis) revealed variable copy number between each sample with no correlation to patient age.
|
Screening of all samples using S. noxia-specific primers revealed slightly more than one third of the total samples (n=35/96 or 37.5%) harbored DNA for this organism (Figure 2). More specifically, 24.1% or the pediatric samples (n=13/54) harbored S. noxia, while 52.4% (n=22/42) tested positive.
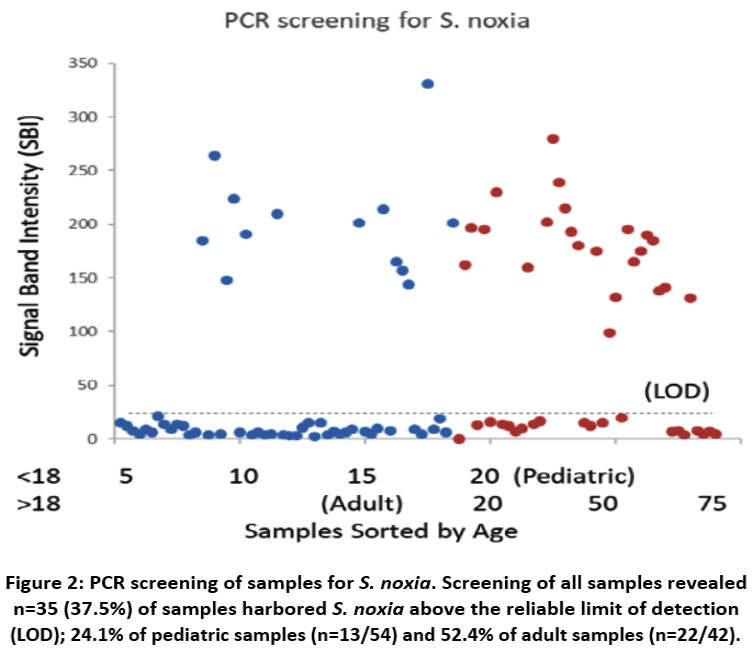 | Figure 2: PCR screening of samples for S. noxia. Screening of all samples revealed n=35 (37.5%) of samples harbored S. noxia above the reliable limit of detection (LOD); 24.1% of pediatric samples (n=13/54) and 52.4% of adult samples (n=22/42).
|
Discussion
Based upon the paucity of evidence regarding oral prevalence, the objective of was to evaluate S. noxia prevalence by sampling saliva from the oral cavity to screen for this pathogen. Using an existing saliva repository, this retrospective study was able to analyze samples from a dental school patient population using isolated DNA and qPCR screening for the presence of S. noxia.
These data confirm previous reports from this group regarding the high oral prevalence among adult patients.15 However, the presence of this organism in pediatric populations was not previously observed in other studies from this group.16 This may suggest that studies, such as this current study, with larger sample sizes may be sufficient to adequately assess the oral prevalence of this organism among pediatric populations that may not exhibit similar microbial profiles as adult populations.
Despite these significant findings, this study has limitations that must also be considered. For example, this was a retrospective study involving a one-time (cross sectional) sampling of pediatric and adult patients. Therefore, no temporal information regarding the timing or duration of this organism was available for analysis. In addition, due to the retrospective nature of this study, only basic demographic information that was previously collected was available to the study authors (Sex, Age, Race / Ethnicity) – therefore no other oral or systemic health information, such as body mass index (BMI), periodontal pocket depth (PPD) or decayed, missing, filled teeth (DMFT) were available.
Conclusions
However, this study provides novel information regarding the oral prevalence of S. noxia among both pediatric and adult populations from a dental school population. These data are an important part of the overall epidemiologic analysis of this organism and may provide some initial information regarding the risk for periodontal or other health issues related to the presence among these populations.
Acknowledgements
The authors would like to thank Dr. Cody Hughes and the Department of Advanced Education, Pediatric program as well as Dr. Jeffrey Ebersole and the Office of Research at the University of Nevada, Las Vegas – School of Dental Medicine for funding and support to complete this project.
Competing Interests
The authors have declared that no competing interests exist.
Author Contributions
KK was responsible for sample collection and experimental protocol. KK and RD were responsible for DNA isolation and PCR screening, as well as project design and funding. RD, KK and KH participated in data analysis and manuscript preparation.
References
- Cornejo Ulloa P, van der Veen MH, Krom BP. Review: modulation of the oral microbiome by the host to promote ecological balance. Odontology. 2019 Feb 4. doi: 10.1007/s10266-019-00413-x. [Epub ahead of print] Review. PMID: 30719639
CrossRef - Lynge Pedersen AM, Belstrøm D. The role of natural salivary defences in maintaining a healthy oral microbiota. J Dent. 2019 Jan;80 Suppl 1:S3-S12. doi: 10.1016/j.jdent.2018.08.010. PMID: 30696553
CrossRef - Baker JL, Edlund A. Exploiting the Oral Microbiome to Prevent Tooth Decay: Has Evolution Already Provided the Best Tools? Front Microbiol. 2019 Jan 11;9:3323. doi: 10.3389/fmicb.2018.03323. eCollection 2018. PMID: 30687294
CrossRef - Shah S. Salivaomics: The current scenario. J Oral Maxillofac Pathol. 2018 Sep-Dec;22(3):375-381. doi: 10.4103/jomfp.JOMFP_171_18. Review. PMID: 30651683
- Karpiński TM. Role of Oral Microbiota in Cancer Development. Microorganisms. 2019 Jan 13;7(1). pii: E20. doi: 10.3390/microorganisms7010020. Review. PMID: 30642137
CrossRef - Ebersole JL, Dawson DA 3rd, Emecen Huja P, Pandruvada S, Basu A, Nguyen L, Zhang Y, Gonzalez OA. Age and Periodontal Health - Immunological View. Curr Oral Health Rep. 2018 Dec;5(4):229-241. doi: 10.1007/s40496-018-0202-2. Epub 2018 Nov 7. PMID: 30555774
CrossRef - Fonkou MD, Dufour JC, Dubourg G, Raoult D. Repertoire of bacterial species cultured from the human oral cavity and respiratory tract. Future Microbiol. 2018 Nov;13:1611-1624. doi: 10.2217/fmb-2018-0181. Epub 2018 Nov 12. PMID: 30417656
CrossRef - Tanner AC. Anaerobic culture to detect periodontal and caries pathogens. J Oral Biosci. 2015 Feb;57(1):18-26. PMID: 25678835
CrossRef - López R, Dahlén G, Retamales C, Baelum V. Clustering of subgingival microbial species in adolescents with periodontitis. Eur J Oral Sci. 2011 Apr;119(2):141-50. doi: 10.1111/j.1600-0722.2011.00808.x. Epub 2011 Mar 3. PMID: 21410554
CrossRef - Colombo AP, Boches SK, Cotton SL, Goodson JM, Kent R, Haffajee AD, Socransky SS, Hasturk H, Van Dyke TE, Dewhirst F, Paster BJ. Comparisons of subgingival microbial profiles of refractory periodontitis, severe periodontitis, and periodontal health using the human oral microbe identification microarray. J Periodontol. 2009 Sep;80(9):1421-32. doi: 10.1902/jop.2009.090185. PMID: 19722792
CrossRef - Faveri M, Mayer MP, Feres M, de Figueiredo LC, Dewhirst FE, Paster BJ. Microbiological diversity of generalized aggressive periodontitis by 16S rRNA clonal analysis. Oral Microbiol Immunol. 2008 Apr;23(2):112-8. doi: 10.1111/j.1399-302X.2007.00397.x. PMID: 18279178
CrossRef - Goodson JM, Groppo D, Halem S, Carpino E. Is obesity an oral bacterial disease? J Dent Res. 2009 Jun;88(6):519-23. doi: 10.1177/0022034509338353. PMID: 19587155
CrossRef - Cruz P, Mehretu AM, Buttner MP, Trice T, Howard KM. Development of a polymerase chain reaction assay for the rapid detection of the oral pathogenic bacterium, Selenomonas noxia. BMC Oral Health. 2015 Aug 14;15:95. doi: 10.1186/s12903-015-0071-1. PMID: 26272608
CrossRef - Dahlén G, Leonhardt A. A new checkerboard panel for testing bacterial markers in periodontal disease. Oral Microbiol Immunol. 2006 Feb;21(1):6-11. PMID: 16390335
CrossRef - McDaniel S, McDaniel J, Tam A, Kingsley K. Howard KM. Oral Microbial Ecology of Selenemonas noxia and Scardovia wiggsiae. Microbiology Research Journal International 2017, 21(3) 1-8. DOI : 10.9734/MRJI/2017/36110
CrossRef - Bui Q, Nguyen C, McDaniel J, McDaniel S, Kingsley K, Howard KM. Selenomonas noxia screening among pediatric patient samples: a pilot study. J Oral Heal Dent Care 2017, 1:1009; Open Access
CrossRef
Abbreviations
Institutional Review Board (IRB)
Office for the Protection of Human Research Subjects (OPRS)
University of Nevada, Las Vegas (UNLV), deoxyribonucleic acid (DNA)
quantitative real-time polymerase chain reaction (qPCR)
American Type Culture Collection (ATCC)
glyceraldehyde 3-phosphate dehydrogenase (GAPDH)
limit of detection (LOD)
signal band intensity (SBI)
body mass index (BMI)
periodontal pocket depth (PPD)
decayed
missing
filled teeth (DMFT)





